Download

1 / 5
50 likes | 51 Views
The natural history of Translocation renal cell carcinomas (tRCC) is variable from indolent behaviors to aggressive disease that demonstrates lymph node and widespread metastasis. Translocation renal cell carcinomas (TRCC) represent 1% to 5% of all cases of renal cell carcinoma (RCC). We sought to characterize the associations between age at presentation of tRCC patients and stage, grade, survival and recurrence of the disease in Middle Eastern institution. Materials and methods: Retrospective review of clinical and pathological data from a single institution for 23 patients diagnosed with tRCC between 2005 and 2017.

E N D
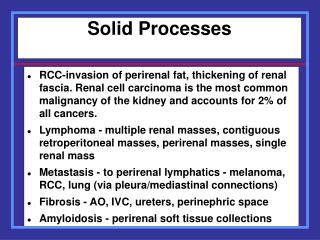
JournalofOncologyResearch&Treatments Journal of Oncology Research and Treatments Al-Daghmin et al., J Oncol Res Treat 2019, 4:1 Review Article Open Access Does Age Affect the Outcomes of Translocation Renal Cell Carcinoma? A Retrospective Analysis from A Middle Eastern Cohort Ali Al-Daghmin*, Sohaib Alhamss, Weam Al-Qasem, Khloud Al-Qasem, Lujain Al-Omari, Hani Al-Najjar and Duaa DAhbour Department of Surgery, King Hussein Cancer Center Surgery, Jordan Abstract Background: The natural history of Translocation renal cell carcinomas (tRCC) is variable from indolent behaviors to aggressive disease that demonstrates lymph node and widespread metastasis. Translocation renal cell carcinomas (TRCC) represent 1% to 5% of all cases of renal cell carcinoma (RCC). Objectives: We sought to characterize the associations between age at presentation of tRCC patients and stage, grade, survival and recurrence of the disease in Middle Eastern institution. Materials and methods: Retrospective review of clinical and pathological data from a single institution for 23 patients diagnosed with tRCC between 2005 and 2017. Patients were categorized into two group based on age group 1 (>40 years) and group 2 (≤ 40 years). We evaluated the association between tumor grade, gender, disease free survival (DFS), overall survival (OS) and age. Results: The tumor was on the right kidney in 52.2% of the patients, and bilateral in one patient. Ten patients (43.5%) were above 40 years of age, and 13 patients (56.5%) were less than or equal to 40 years old regarding the tumor characteristics, the mean tumor size was 9 cm; 4 patients (17.3%) had pathologic T1, seven patients (30.4%) had pathologic T2, 10 patients (43.4%) had pathologic T3 or more and two patients (8.7%) had no surgery. Eleven patients (47.8%) had lymph node dissection for clinically enlarged lymph nodes and seven (64%) of them had lymph nodes metastasis. Nineteen patients (83%) underwent radical nephrectomy and two (8%) had partial nephrectomy. Bilateral renal tumors were managed with left radical and right partial nephrectomy. There were no differences in DFS in patients above and below 40 years of age. No statistically significant associations between Disease-Free survival, gender, pathologic T staging, overall survival and age. Conclusion: tRCC has variable clinical behavior from indolent to aggressive disease. Age may not affect this clinical behavior. Keywords: Renal cell carcinoma; Translocation renal cell carcinomas; Microphthalmia-associated transcription Introduction Renal cell carcinomas (RCCs) are a heterogeneous group of tumors which account for around 90% of all adult renal malignancies [1]. The most common subtypes are clear cell (60-75%), followed by papillary (10-15%), chromophobe (5%) and collecting duct carcinoma [2]. Recent advances in the understanding of molecular alterations implicated in the pathogenesis of RCC have led to the development of a new sub- classification of these tumors [3]. Translocation renal cell carcinoma (tRCC) is a newly recognized subtype of RCC with chromosomal translocations involving TFE3 (Xp11.2) or, less frequently, TFEB (6p21) [4]. Microphthalmia-associated transcription (MiT) family tRCC entails Xp11 tRCC and t (6;11) RCC. Xp11 tRCC and t (6;11) RCC are also known as TFE3- and TFEB-rearranged RCC, respectively. TFE3 and TFEB belong to the MiT family that regulates melanocyte and osteoclast differentiation. TFE3- and TFEB-rearranged RCC show distinguished clinicopathological and immunohistochemical features [5]. Xp11 tRCC comprises 20-40% of childhood RCC and about 4% of adult RCC with an average age of 50 years at diagnosis [6,7]. The natural history of Xp11 tRCC is variable from indolent behaviors [8,9] to aggressive disease that demonstrates lymph node and widespread metastasis. Xp11 tRCCs have the potential to metastasize as late as 20-30 years after diagnosis [7,10]. The associations between age, stage, grade of the disease, survival and recurrence of the disease have not been addressed in the literature. The aim of this study is to identify if these associations exist. Materials and Methods Study settings The study was conducted at King Hussein Cancer Centre (KHCC), a comprehensive center that serves cancer patients in both inpatient and outpatient settings. RCC patients receive treatment according to KHCC-clinical practice guidelines (CPG). Approval was gained from the KHCC Institutional Review Board and the KHCC ethics committee. Data for all patients who underwent radical or partial nephrectomy and pathology that revealed tRCC between December 2005 and August 2017 were reviewed retrospectively. Study design All patients underwent staging assessment at the time of diagnosis, including clinical examination, blood tests, chest x-ray and computed tomography (CT) of the abdomen and pelvis. Pathological staging was performed using 2010 TNM classification system. Follow-ups were performed according to KHCC-CPGs, which included laboratory and radiological examinations according to the final TNM stage and tumor grade. Additional imaging was ordered as clinically indicated. For those with metastatic disease, tumors were evaluated by physical examination and CT scans at baseline and every 3 to 6 months. Overall disease responses were documented using RECIST criteria [11]. *Corresponding author: Ali Al-Daghmin, Urologic Oncology & Robotic Surgery Consultant, Surgery Department King Hussein Cancer Center, Jordan, Tel: 00962798917748; E-mail: A_daghamin@hotmail.com Received December 24, 2018; Accepted December 31, 2018; Published January 07, 2019 Citation: Al-Daghmin A, Alhamss S, Al-Qasem W, Al-Qasem K, Al-Omari L, et al.(2019) Does Age Affect the Outcomes of Translocation Renal Cell Carcinoma? A Retrospective Analysis from A Middle Eastern Cohort J Oncol Res Treat 4: 128. Copyright: © 2019 Al-Daghmin A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. J Oncol Res Treat, an open access journal Volume 4 • Issue 1 • 1000128
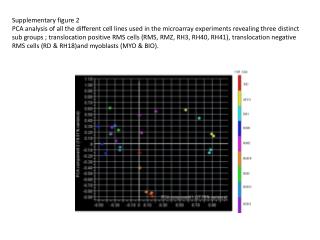
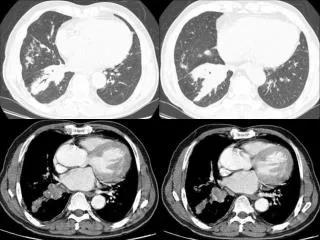
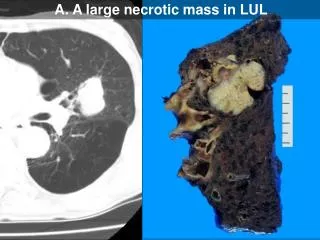
Citation: Al-Daghmin A, Alhamss S, Al-Qasem W, Al-Qasem K, Al-Omari L, et al.(2019) Does Age Affect the Outcomes of Translocation Renal Cell Carcinoma? A Retrospective Analysis from A Middle Eastern Cohort J Oncol Res Treat 4: 128. Page 2 of 5 Statistical analysis The Chi-squared test was used to identify associations between results, responses, and demographics. The strength of associations was assessed by calculating odds ratios (ORs) and 95% confidence intervals. Relations between categorical and continuous variables were evaluated in independent t tests. Cross-tabulation was used to explore associations between categorical data, and chi-squared tests were used to assess the statistical significance of associations. P values less than 0.05 were considered statistically significant. Results Clinical characteristics Twenty-three patients were identified, 15 (65%) of the patients were males. The mean age at diagnosis was 37 years. The majority of the patients (65%) were diagnosed incidentally during abdominal imaging for other indications. The remaining 35% suffered from pain, gross hematuria, metastasis, abdominal distension or weight loss at the time of the first presentation. Patients’ characteristics are shown in Table 1. TFE3 stain was performed for tumors with histological features suggestive of tRCC, like papillary architecture and clear to eosinophilic cytoplasm. The diagnosis of Xp11 tRCC was confirmed by immunohistochemistry (IHC) analysis for nuclear TFE3 staining. Xp11.2 tRCC was analyzed by IHC staining to detect TFE3 in each tumor and tissue microarray block (catalog No. sc5958; Santa Cruz Biotechnology, Santa Cruz, CA, USA). Angiogenesis markers IHC analysis of the tumor tissue samples was performed by using the Ventana XT auto immunostainer (Roche, San Francisco, CA, USA) with the Optiview Dab Detection Kit (Roche) according to the manufacturer’s instructions. The results were independently evaluated by two specialized pathologists blind to the clinical data. The Fuhrman nuclear grading system, which uses a four point multi-parametric scale based on nuclear features, size, shape, color, and nucleolar prominence was used [12] as shown in Figures 1-3. Data including the patients’ characteristics, clinical manifestations, surgical techniques, pathological findings, radiology, and clinical outcomes was collected. Response to treatment based on cancer-specific survival (CCS), overall survival (OS) and progression-free survival (PFS) were analyzed. Patients were categorized into two group based on age group 1 (>40 years) and group 2 (≤ 40 years) and association between tumor grade, sex, disease free survival (DFS) and age were studied across groups. The tumor was on the right kidney in 52.2% of the patients, and bilateral in one patient. Ten patients (43.5%) were above 40 years of age, and 13 patients (56.5%) were less than or equal to 40 years old. Regarding the tumor characteristics, the mean tumor size was 9 cm; 4 patients (17.3%) had pathologic T1, seven patients (30.4%) had pathologic T2, 10 patients (43.4%) had pathologic T3 or more and two patients (8.7%) had no surgery and thus were not evaluated for pathologic T staging. Eleven patients (47.8%) had lymph node dissection for clinically enlarged lymph nodes and seven (64%) of them had lymph nodes metastasis. Patients were categorized into two group based on age group 1 (<40 years) and group 2(<=40 years). Tumor T stage distribution among groups are shown in Table 2. Figure 1: The results were independently evaluated by two specialized pathologists blind to the clinical data. Patient Number Age at Presentation (years) 41 36 58 33 13 2 26 51 38 48 31 25 43 44 33 22 41 35 32 47 43 66 37 Sex Presenting Symptom Laterality 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Male Male Male Male Female Female Male Male Male Male Female Female Male Female Female Female Male Male Male Male Male Male Female Incidental Diagnosis Incidental diagnosis Incidental diagnosis Incidental diagnosis Incidental diagnosis Abdominal Distension Fatigue and hematuria Incidental diagnosis Incidental diagnosis Incidental diagnosis Incidental diagnosis Incidental diagnosis Incidental diagnosis Incidental diagnosis Abdominal Pain Loin Pain Neck mass Hematuria Incidental diagnosis Incidental diagnosis Incidental diagnosis Loin pain and hematuria Fatigue, weight loss and loin pain Left Right Bilateral Right Right Right Left Right Left Right Right Left Right Left Left Right Right Left Right Left Right Left Left Figure 2: The Fuhrman nuclear grading system, which uses a four point multi-parametric scale based on nuclear features, size, shape, color, and nucleolar prominence was used. Figure 3: The Fuhrman nuclear grading system, which uses a four point multi-parametric scale based on nuclear features, size, shape, color, and nucleolar prominence was used. Table 1: Demographic data of patient population. J Oncol Res Treat, an open access journal Volume 4 • Issue 1 • 1000128
Citation: Al-Daghmin A, Alhamss S, Al-Qasem W, Al-Qasem K, Al-Omari L, et al.(2019) Does Age Affect the Outcomes of Translocation Renal Cell Carcinoma? A Retrospective Analysis from A Middle Eastern Cohort J Oncol Res Treat 4: 128. Page 3 of 5 Patient Number 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Disease-Free Period Postoperatively No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis 3 months 5 months 3 years 3 years No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis 5 years Metastasis on presentation Metastasis at presentation No recurrence or metastasis No recurrence or metastasis Metastasis on presentation No recurrence or metastasis No recurrence or metastasis Site of Recurrence No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis Local recurrence Lung Bone, soft tissue, adrenal glands, peritoneum Lung No recurrence or metastasis No recurrence or metastasis No recurrence or metastasis Regional lymph nodes Bilateral lung, left cervical, mediastinal and para-aortic Lymph nodes Lung and retroperitoneal lymph nodes No recurrence or metastasis No recurrence or metastasis Multiple para-aortic lymph nodes No recurrence or metastasis No recurrence or metastasis Table 2: Disease-free period and site of recurrence and metastasis. Surgical intervention Nineteen patients (83%) underwent radical nephrectomy and two (8%) had partial nephrectomy. Bilateral renal tumors were managed with left radical and right partial nephrectomy. Eighteen patients (78%) had an open approach and three patients (13%) had a laparoscopic approach. Eight patients (35%) had metastasis, and three of the eight patients had metastasis at the time of diagnosis. Six patients (26%) received sunitinib for their metastatic disease, and one of them had a complete response with a disease free period of 18 months. Four patients had a stable disease for an average of 19 months, and only one had disease progression without any response (Table 3). There were no differences in DFS in patients above and below 40 years of age. No statistically significant associations between disease-free period postoperatively, sex, pathologic T staging, overall survival and age were found across the groups, using 40 years as a cut point (Figures 4 and 5). Follow up Three patients died during follow-up time; one patient died 4 months after surgery, one 21 months after surgery (both due to metastasis) and one died of brain hemorrhage. The mean follow-up time is 35 months, and 3-year disease overall free survival was 75%. Discussion The median age at diagnosis of RCC is approximately 64, according to the 2003 to 2007 National Cancer Institute (NCI) and the Surveillance, Epidemiology and End Results (SEER) Cancer Statistics Review. RCC is unusual in patients under 40 years of age and is rare in children [13- 15]. tRCC, is a distinct variant of RCC and is associated with fusion of the TFE3 gene to other genes located on chromosome Xp11.2 [8,9,16]. Xp tRCC was initially thought to be a malignancy of pediatrics and young adults. However, more recent data has increasingly identified this tumor in older adults as well [17]. Adequate immunohistochemical workup is not routinely done for adults with RCC, which results in most cases of adult tRCC misdiagnosed as conventional [18]. T stage Not available T1 T1b T2 T2a T2b T3 T3a T3b T4 Total 2 Age<=40 2 Age>40 0 3 1 2 3 1 2 4 3 2 2 (18%) 0 1 (9%) 2 (18%) 1 (9%) 1 (9%) 1 (9%) 2 (18%) 1 (9%) 1 (10%) 1 (10%) 1 (10%) 1 (10%) 0 1 (10%) 3 (30%) 1 (10%) 1 (10%) Table 3: T staging of patients (n=23). Figure 4: No statistically significant associations between Disease-Free Period postoperatively, sex, pathologic T staging, overall survival and age were found across the groups, using 40 years as a cut point. Furthermore, the similar gross and histological findings to other RCCs also contributed to the underestimation of tRCC frequency in adults [19]. J Oncol Res Treat, an open access journal Volume 4 • Issue 1 • 1000128
Citation: Al-Daghmin A, Alhamss S, Al-Qasem W, Al-Qasem K, Al-Omari L, et al.(2019) Does Age Affect the Outcomes of Translocation Renal Cell Carcinoma? A Retrospective Analysis from A Middle Eastern Cohort J Oncol Res Treat 4: 128. Page 4 of 5 T staging, and overall survival in patients with tRCC treated in KHCC. No significant associations were found across the groups. This study is limited by a retrospective design and the absence of long-term follow-up. Furthermore, the small sample size makes it difficult to draw a definitive conclusion regarding associations between age and the factors studied. Conclusion tRCC, is a variant of RCC with unique characteristics. tRCC has variable clinical behavior from indolent to aggressive disease. Age may not affect this clinical behavior. Future studies with larger sample size and a longer follow up period is required. References 1. Low G, Huang G, Fu W, Moloo Z, Girgis S (2016) Review of renal cell carcinoma and its common subtypes in radiology. WJR 8: 484. Figure 5: No statistically significant associations between Disease-Free Period postoperatively, sex, pathologic T staging, overall survival and age were found across the groups, using 40 years as a cut point. 2. Rini BI, Campbell SC, Escudier B (2009) Renal cell carcinoma. The Lancet 373: 1119-1132. 3. Linehan WM, Bratslavsky G, Pinto PA, Schmidt LS, Neckers L, et al. (2010) Molecular diagnosis and therapy of kidney cancer. Annu Rev Med 61: 329-343. Translocation carcinoma tens to occur at a younger age compared with other RCCs: In our study the mean age at diagnosis is 37 years and is more common in males (65%) than in females. Nevertheless, current data depending on many cohort studies as well as some meta-analyses show that the course of tRCC is more indolent in pediatric populations. Adults tend to present with advanced stage and distant metastases and thus have a poorer prognosis [17,20]. The treatment of Xp11.2 tRCC remains a major challenge for health care providers. Many advances in the treatment of clinically localized and metastatic RCC disease have been accomplished [21]. This is not the case in tRCC management due to the small number of patients to run clinical trials. Thirty cases of t(6;11) RCC were reported in the International Society of Urological Pathology Conference. Of these, the majority of pediatric cases were indolent with recurrence in only 17% of them. Most of the adult population in the same study presented with metastasis or pursued an aggressive clinical course causing death [22]. Another study which focused on regional lymph node metastasis as a prognostic factor for tRCC showed that regional lymph node metastasis in pediatrics doesn’t necessarily predict poor prognosis as it nearly does in adults [8]. Another multivariate analysis by Peckova et al. demonstrated that the more aggressive t(6,11) RCC appeared to affect older patients (mean age of 45.2 years) rather than younger patients (mean age of 31.5 years) [23]. The management of clinically localized Xp11.2 tRCC is similar to general RCC guidelines [24]. Currently, there is no standard treatment for patients with MiT family tRCC. Most studies depend on the PFS, CSS and OS as indicators of the efficiency of different treatment modalities. Currently, the most favorable outcomes have been reported with patients who undergo a radical nephrectomy and lymph node dissection before the development of metastasis. However, the true challenge lies in the postoperative follow-up process; special follow-up protocols are seemingly promising in improving the quality of life of tRCC adult patients and in prolongation of the three mentioned parameters [25]. Future studies will focus on genomic technologies to identify prognostic factors and therapeutic targets in tRCC. One study found that high chromosome copy number alterations in Xp11 tRCC are associated with aggressive behavior [24]. Another found that chromosome 17q gain correlated with older age and worse outcome which corroborates the effect of age reported by Ellis et al. [10]. The scope of this study is to address the association between age (> or ≤ 40 years) and disease free period postoperatively, sex, pathologic 4. Zhong M, De Angelo P, Osborne L, Mondolfi P, Geller M, et al. (2012) Translocation renal cell carcinomas in adults: A single institution experience. Am J Surg Pathol 36: 654. 5. Inamura K (2017) Translocation Renal Cell Carcinoma: An update on clinicopathological and molecular features. Cancers 9: 111. 6. Kmetec A, Jeruc J (2014) Xp 11.2 translocation renal carcinoma in young adults; recently classified distinct subtype. Radiol Oncol 48: 197-202. 7. Sukov WR, Hodge JC, Lohse CM, Leibovich BC, Thompson RH, et al. (2012) TFE3 rearrangements in adult renal cell carcinoma: Clinical and pathologic features with outcome in a large series of consecutively treated patients. Am J Surg Pathol 36: 663-670. 8. Argani P, Antonescu CR, Illei PB, Lui MY, Timmons CF, et al. (2001) Primary renal neoplasms with the ASPL-TFE3 gene fusion of alveolar soft part sarcoma: a distinctive tumor entity previously included among renal cell carcinomas of children and adolescents. Am J Surg Pathol 159: 179-192. 9. Argani P, Antonescu CR, Couturier J, Fournet JC, Sciot R, et al. (2002) PRCC- TFE3 renal carcinomas: morphologic, immunohistochemical, ultrastructural, and molecular analysis of an entity associated with the t (X; 1)(p11. 2; q21). Am J Surg Pathol 26: 1553-1566. 10. Ellis CL, Eble JN, Subhawong AP, Martignoni G, Zhong M, et al. (2014) Clinical heterogeneity of Xp11 translocation renal cell carcinoma: impact of fusion subtype, age, and stage. Mod Pathol 27: 875. 11. Therasse P, Eisenhauer E, Verweij J (2006) RECIST revisited: a review of validation studies on tumour assessment. EJC 42: 1031-1039. 12. Fuhrman SA, Lasky LC, Limas C (1982) Prognostic significance of morphologic parameters in renal cell carcinoma. Am J Surg Pathol 6: 655-663. 13. Siegel R, Ward E, Brawley O, Jemal A (2011) Cancer statistics 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 61: 212-236. 14. Siemer S, Hack M, Lehmann J, Becker F, Stöckle M (2006) Outcome of renal tumors in young adults. J Urol 175: 1240-1244. 15. Thompson RH, Ordonez MA, Iasonos A, Secin FP, Guillonneau B, et al. (2008) Renal cell carcinoma in young and old patients-is there a difference? J Urol 180: 1262-1266. 16. Malouf GG, Camparo P, Molinié V, Dedet G, Oudard S, et al. (2011) Transcription factor E3 and transcription factor EB renal cell carcinomas: clinical features, biological behavior and prognostic factors. J Urol 185: 24-29. 17. Meyer PN, Clark JI, Flanigan RC, Picken MM (2007) Xp11.2 translocation renal cell carcinoma with very aggressive course in five adults. Am J Clin Pathol 128: 70-79. 18. Argani P, Olgac S, Tickoo SK, Goldfischer M, Moch H, et al. (2007) Xp11 J Oncol Res Treat, an open access journal Volume 4 • Issue 1 • 1000128
Citation: Al-Daghmin A, Alhamss S, Al-Qasem W, Al-Qasem K, Al-Omari L, et al.(2019) Does Age Affect the Outcomes of Translocation Renal Cell Carcinoma? A Retrospective Analysis from A Middle Eastern Cohort J Oncol Res Treat 4: 128. Page 5 of 5 translocation renal cell carcinoma in adults: expanded clinical, pathologic, and genetic spectrum. Am J Surg Pathol 31: 1149-1160. 22. Pecciarini L, Cangi MG, Lo Cunsolo C, Macri’ E, Dal Cin E, et al. (2007) Characterization of t (6; 11) (p21; q12) in a renal‐ cell carcinoma of an adult patient. Genes, Chromosomes and Cancer 46: 419-426. 19. Cutruzzula P, Cahn D, Kivlin D, Tong C, Edwards D, et al. (2017) A Review of Translocation T(6;11) Renal Cell Carcinoma Tumors in the Adult Patient. Curr Urol 10: 69-71. 23. Peckova K, Vanecek T, Martinek P, Spagnolo D, Kuroda N, et al. (2014) Aggressive and nonaggressive translocation t (6; 11) renal cell carcinoma: comparative study of 6 cases and review of the literature. Ann Diagn Pathol 18: 351-7. 20. Huh H, Jo HA, Yi Y, Kim SH, Moon KC, et al. (2017) Xp11. 2 translocation renal cell carcinoma in the autosomal dominant polycystic kidney disease patient with preserved renal function. Korean J Intern Med 32: 1108. 24. Escudier B, Eisen T, Porta C, Patard J, Khoo V, et al. (2012) Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 23: 765-771. 21. Malouf GG, Camparo P, Oudard S, Schleiermacher G, Theodore C, et al. (2010) Targeted agents in metastatic Xp11 translocation/TFE3 gene fusion renal cell carcinoma (RCC): a report from the Juvenile RCC Network. Annals of oncology: Official Journal of the European Society for Medical Oncology/ ESMO 21: 1834-1838. 25. Aoyagi T, Shinohara N, Kubota-Chikai K, Kuroda N, Nonomura K (2011) Long- term survival in a patient with node-positive adult-onset Xp11. 2 translocation renal cell carcinoma. Urol Int 86: 487-90. J Oncol Res Treat, an open access journal Volume 4 • Issue 1 • 1000128