Download
1 / 1
10 likes | 150 Views
Communication of infection control requirements at a large paediatric hospital. Saari , M.E., Saeed , M.O., Burnham, E., Omar, S., Folkins , C., Chen, S., Chen, J., Robichaud , P., Thomas, R., Swift, M., Bae , J.E., Matlow , A., Wray, R. Introduction. Methods. Response Distributions (EHR).

E N D
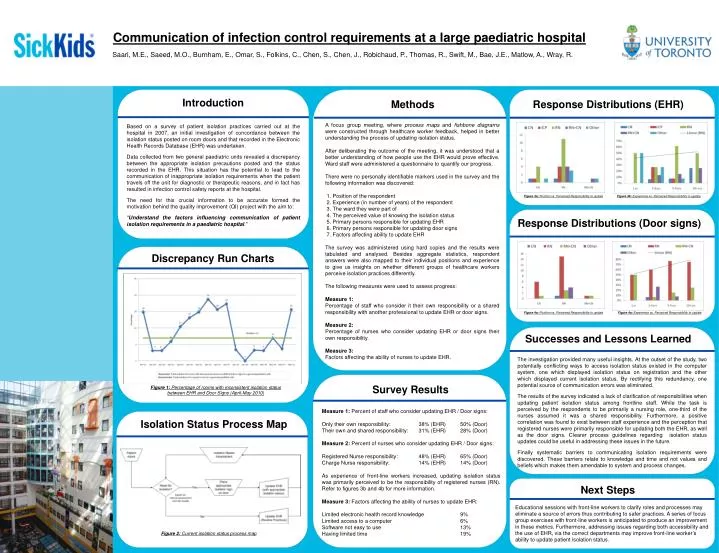
Communication of infection control requirements at a large paediatric hospital Saari, M.E., Saeed, M.O., Burnham, E., Omar, S., Folkins, C., Chen, S., Chen, J., Robichaud, P., Thomas, R., Swift, M., Bae, J.E., Matlow, A., Wray, R. Introduction Methods Response Distributions (EHR) A focus group meeting, where process maps and fishbone diagrams were constructed through healthcare worker feedback, helped in better understanding the process of updating isolation status. After deliberating the outcome of the meeting, it was understood that a better understanding of how people use the EHR would prove effective. Ward staff were administered a questionnaire to quantify our progress. There were no personally identifiable markers used in the survey and the following information was discovered: 1. Position of the respondent 2. Experience (in number of years) of the respondent 3. The ward they were part of 4. The perceived value of knowing the isolation status 5. Primary persons responsible for updating EHR 6. Primary persons responsible for updating door signs 7. Factors affecting ability to update EHR The survey was administered using hard copies and the results were tabulated and analysed. Besides aggregate statistics, respondent answers were also mapped to their individual positions and experience to give us insights on whether different groups of healthcare workers perceive isolation practices differently. The following measures were used to assess progress: Measure 1: Percentage of staff who consider it their own responsibility or a shared responsibility with another professional to update EHR or door signs. Measure 2: Percentage of nurses who consider updating EHR or door signs their own responsibility. Measure 3: Factors affecting the ability of nurses to update EHR. Based on a survey of patient isolation practices carried out at the hospital in 2007, an initial investigation of concordance between the isolation status posted on room doors and that recorded in the Electronic Health Records Database (EHR) was undertaken. Data collected from two general paediatric units revealed a discrepancy between the appropriate isolation precautions posted and the status recorded in the EHR. This situation has the potential to lead to the communication of inappropriate isolation requirements when the patient travels off the unit for diagnostic or therapeutic reasons, and in fact has resulted in infection control safety reports at the hospital. The need for this crucial information to be accurate formed the motivation behind the quality improvement (QI) project with the aim to: “Understand the factors influencing communication of patient isolation requirements in a paediatric hospital.” Figure 3a: Position vs. Perceived Responsibility to update Figure 3b: Experience vs. Perceived Responsibility to update Response Distributions (Door signs) Discrepancy Run Charts Figure 4a: Position vs. Perceived Responsibility to update Figure 4a: Experience vs. Perceived Responsibility to update Successes and Lessons Learned The investigation provided many useful insights. At the outset of the study, two potentially conflicting ways to access isolation status existed in the computer system, one which displayed isolation status on registration and the other which displayed current isolation status. By rectifying this redundancy, one potential source of communication errors was eliminated. The results of the survey indicated a lack of clarification of responsibilities when updating patient isolation status among frontline staff. While the task is perceived by the respondents to be primarily a nursing role, one-third of the nurses assumed it was a shared responsibility. Furthermore, a positive correlation was found to exist between staff experience and the perception that registered nurses were primarily responsible for updating both the EHR, as well as the door signs. Clearer process guidelines regarding isolation status updates could be useful in addressing these issues in the future. Finally systematic barriers to communicating isolation requirements were discovered. These barriers relate to knowledge and time and not values and beliefs which makes them amendable to system and process changes. Survey Results Figure 1: Percentage of rooms with inconsistent isolation status between EHR and Door Signs (April-May 2010) • Measure 1: Percent of staff who consider updating EHR / Door signs: • Only their own responsibility: 38% (EHR) 50% (Door) • Their own and shared responsibility: 31% (EHR) 28% (Door) • Measure 2: Percent of nurses who consider updating EHR / Door signs: • Registered Nurse responsibility: 48% (EHR) 65% (Door) • Charge Nurse responsibility: 14% (EHR) 14% (Door) • As experience of front-line workers increased, updating isolation status was primarily perceived to be the responsibility of registered nurses (RN). Refer to figures 3b and 4b for more information. • Measure 3: Factors affecting the ability of nurses to update EHR: • Limited electronic health record knowledge 9% • Limited access to a computer 6% • Software not easy to use 13% • Having limited time 19% Isolation Status Process Map Next Steps Educational sessions with front-line workers to clarify roles and processes may eliminate a source of errors thus contributing to safer practices. A series of focus group exercises with front-line workers is anticipated to produce an improvement in these metrics. Furthermore, addressing issues regarding both accessibility and the use of EHR, via the correct departments may improve front-line worker’s ability to update patient isolation status. Figure 2: Current isolation status process map