Download
1 / 131
1.37k likes | 1.66k Views
Prevention and promotion in health. A learning tool. Prevention and Promotion in Health: A Learning Tool is licensed under a Creative Commons Attribution- NonCommercial 4.0 International License. Collaborators : Dr Julie Dufort, MD, M.Sc ., FRCPC Dr Catherine Risi, MD, M.Sc

E N D
Prevention and promotion in health A learning tool Prevention and Promotion in Health: A Learning Tool is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Collaborators: Dr Julie Dufort, MD, M.Sc., FRCPC Dr Catherine Risi, MD, M.Sc Mélanie Ann Smithman (translation) Authors: Geneviève Bustros-Lussier, MD David-Martin Milot, MD Andréanne Roy, MD Residents in Public Health and PreventiveMedicine Université de Sherbrooke Toolcreated in January 2014
Disclaimer The authors are not responsible for errors or omissions or for any consequences from application of the information in this Learning Tool and make no warranty, expressed or implied, with respect to the currency, completeness, or accuracy of the contents of the publication. Application of the information in a particular situation remains the professional responsibility of the practitioner and reader.
Please note thatyouneed to be in "slideshow" mode in order for the interactive parts of thistool to workproperly. Enjoy!
This training tool is also available in French at your convenience.
ContenT This training tool is meant for clerkship students enrolled in Canadian medical schools It consists of the following: The vignettes may be completed with a supervisor or on your own.
Introduction At the end of this training, you should be able to: • Illustrate the concepts of disease prevention and health promotion; • Explain the role of public health and preventive medicine physicians with respect to disease prevention and health promotion; • Identify strategies to apply disease prevention and health promotion to your future clinical practice.
Introduction First of all, a few definitions: Prevention: Disease prevention covers actions to prevent the occurrence of disease, such as risk factor reduction, and also to arrest its progress and reduce its consequences once established. Health Promotion: Activities that aims to enhance health by education, by organizational, economic and political interventions to support behavioural changes conducive to health. “Glossary”. AFMC Primer on Population Health, The Association of Faculties of Medicine of Canada, http://phprimer.afmc.ca/Glossary (retrievedJanuary 2014) Permit : Creative Commons BY-NC-SA
Introduction The concepts of disease prevention and health promotion overlap. In fact, the aim of health promotion includes, but also goes beyond, preventing disease: it seeks, in addition, to strengthen the skills and resiliency of individuals and of community groups. The concepts of disease prevention and health promotion will be illustrated throughout this training. “Glossary”. AFMC Primer on Population Health, The Association of Faculties of Medicineof Canada, http://phprimer.afmc.ca/Glossary (retrievedJanuary 2014) Permit : Creative Commons BY-NC-SA
Quiz Before exploring the applications of promotion and prevention in depth, here is a quiz that will help you answer a question that is certainly on your mind : Do you have what it takes to be a public health and preventive medicine physician? (Click on the image to take the quiz)
Quiz Click on the image with your score*: 0 to 19 20 to 39 40 to 60 *Please note that a higher score does not mean a better score.
Quiz You are a “bandage” type of doctor As a doctor, treating disease is at the core of your work. While it is difficult to be against the old adage “an ounce of prevention is worth a pound of cure”, when a patient is in front of you, your main goal is to address problems. Although treating disease is essential, it has also been shown that clinical prevention is important both for patients and for reducing the costs and ensuring the sustainability of the health care system. You would benefit from this training tool by seeing how you could integrate the preventive aspect into your clinical practice. After all, chronic diseases are largely avoidable and effective prevention strategies exist. As a health professional, you certainly have a role to play in this area. What do you think ? Click here to continue
Quiz You are a “protective helmet” type of doctor It is clear to you that some health problems are avoidable. You seem committed to disease prevention. You probably take advantage of each opportunity to offer advice, screening, preventive medication and vaccines to your patients. Moreover, you organize your workplace’s clinical environment to foster the integration of preventive clinical practices. You firmly believe in the individual approach to disease prevention. The integration of prevention in clinical practice is important, but it has its limits. In fact, your patients are not entirely responsible for their lifestyles: a number of factors including those linked to social and physical environments influence them. This training tool could help you understand why your patients do not always make healthy lifestyle choices and do not follow all of your recommendations. You will gain a better understanding of the determinants that impact your patients’ health and how we can act. Click here to continue
Quiz You are a “supportiveenvironments” type of doctor It is clear to you that most health problems are partially avoidable if we create physical, social and political environments that are supportive of health. You seem naturally interested in understanding why one population has more health problems compared to another. This type of thinking makes up the foundation of the population-based approach to disease prevention and brings us to address the causes of problems by tackling the determinants of health. This training tool will provide examples of broad prevention and promotion strategies that can be implemented to improve the health of the population. You might even find simple ways to integrate those concepts into your practice or life. Have you ever considered a career in public health? Click here to continue
Quiz In summary, imagine the following situation : A child riding a bicycle falls because of a pothole. Dr. Bandage would treat the child. Dr. Protective Helmet would tell the child to be more careful and would suggest the child ride his bicycle on safer roads. Dr. Supportive Environments would instead wonder if potholes cause a significant number of accidents. If so, he would wonder how potholes come about and how to mitigate them.
Introduction According to their respective approaches, these doctors have different positions on the following continuums: To maintainhealth Dr. Protective Helmet Dr. Supportive Environments Individual-centered Population-based Dr. Bandage To restore health or to alleviatedisease and itsconsequences Inspired by Kennedy et al., DSP Saguenay, Lac St-Jean, 2003
introduction One of these continuums relates to the purpose of the approach taken: To maintainhealth For healthy people For sick people To restore health or to alleviatedisease and itsconsequences Inspired by Kennedy et al., DSP Saguenay, Lac St-Jean, 2003
introduction Health promotion and disease prevention mainly aim to maintain health. To maintainhealth Health Promote Risk Prevent Disease Cure Chronicity Treat To restore health or to alleviatedisease and itsconsequences Inspired by Kennedy et al., DSP Saguenay, Lac St-Jean, 2003
introduction The other continuum relates to the health approach’s subject of interest: The Individual The Community • Theirimmediateenvironment • Theirfamilies • Theirfriends • Etc. • The region • The neighborhood • The age group • The risk group • Etc. Individual-centered Population-based Inspired by Kennedy et al., DSP Saguenay, Lac St-Jean, 2003
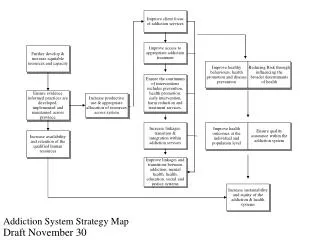
vignettes As shown in the diagram, health approaches may be individual or population-based. The process used in either case remains similar. Here are a few examples: Medicalhistory and physicalexamination Notifiabledisease surveillance Environmentalriskassessment Laboratoryexamination Imaging Outbreak investigation Mass screening Diagnostic tests Opportunistic screening Monitoring healthstatus and determinants of health
Vignettes Programs, projects, promotion, prevention and protection activities Recommendations and prescriptions Legislation and regulation support Evidence-based Evidence-based Follow-up on investigation and treatment Program, project and activityevaluation Ongoing monitoring of the population’shealthstatus Yearlyfollow-up Inspired by Kennedy et al. DSP Saguenay, Lac St-Jean, 2003
Vignettes The difference between these two approaches lies mainly in the unique vision and expertise of each of them. Note that, typically, a clinical physician will have an individual-centered approach while the public health and preventive medicine physician will have a population-based approach. The patient The population Inspired by Kennedy et al. DSP Saguenay, Lac St-Jean, 2003
Vignettes Health promotion and disease prevention can be integrated to each approach. However, disease prevention can be easier to apply and more common in the individual setting. It is at the heart of prevention in clinical practice. The first vignette presents a case in which the individual centered approach was put forth. Many concepts, specific to this type of approach, such as prevention in clinical practice, will be discussed.
vignettes Note that the following vignettes can be completed in two ways. 1) In interaction with a supervisor • The questions will be asked by the supervisor (the resident in charge of the public health and preventive medicine internship). Therefore, it is now time to turn off your computer and play a sport. You will look at the vignettes with your supervisor at a time set aside for this task. 2) In self-learning • Answer the questions that will be asked by yourself and compare your answers to those presented.
Vignette no. 1 Individual-centered approach
Objectives Upon completion of this activity, the participantwill be able to : • Explain the public health and preventive medicine physician’s role in the individual-centered approach to disease prevention and health promotion; • Illustrate the concepts of disease prevention and health promotion; • Identify strategies to apply disease prevention and health promotion at the individual level. Click here to start
Background information You are Dr. Protective Helmet, a physician in a clinic. Ms. Sweet Tooth, 35 years old, comes to see you for her Pap test which is “due”. Since you do not know the patient, you ask her various questions on her personal and family history. Her history is unremarkable. She lives with her spouse and her 4-year-old son and works as a cashier in a grocery store.
Background information Lifestyle She has been smoking a pack a day for the last 14 years. She does very little exercise and her leisure activities are rather sedentary. She stands a lot for work. She eats about 4 servings of fruit and vegetables a day. Contraception et sexual health She has had an IUD for 3 years. She has been with the same partner for 7 years. Screening Her last PAP test was done 2 years ago and her STI screening is up-to-date: it was done during her last pregnancy. She has not had other partners since and neither has her spouse.
Question What is the purpose of asking Ms. Sweet Tooth all of these questions?
ANSWER The purpose of these questions is to find out more about Ms. Sweet Tooth and to guide your preventive clinical practice according to this patient’s characteristics.
Question What is prevention in clinical practice?
Answer Prevention in clinical practice combines a set of various types of effective individual interventions offered in a clinical setting, for example: • counseling on lifestyle choices and habits, • screening or identifying cases of certain diseases or risk factors, • immunization, • chemoprophylaxis (prescription of medication for preventive purposes). MSSS (2008), Programme national de santé publique 2003-2012 - updated 2008, Québec, 103p.
Question How do we know if a preventive clinical practice is recommended?
answer Many expert groups issue guidelines on prevention in clinical practice based on the evidence available. The independence of expert groups and the quality of the evidence may vary: • Independent specialized sources E.g.: Canadian Task Force on Preventive Health Care (CTFPHC), Cochrane Collaboration, U.S. Preventive Services Task Force, etc.; • Health professionals’ associations E.g. : Society of Obstetricians and Gynaecologists of Canada; • Associations dedicated to a certain disease or approach E.g. : Canadian Diabetes Association; • Expert groups and scholarly societies E.g. : On topics such as hypertension, lipids; • Pharmaceutical industry and other private interests.
answer Hence, there may be discrepancies between guidelines for the same preventive practice, in particular due to: • the date of the guideline; • selected studies; • methodology; • the classification of levels of evidence; • the social context to which it is being applied. Source: Roy, A., Groulx, S., Dufort, J., Bélanger, H., Risi, C., Sissoko, H., Paquin, P., Lévesque, M. (2013), "Apprentissage au raisonnement clinique (ARC) en Prévention clinique des maladies chroniques : Activité complémentaire au stage d’externat en santé communautaire," Faculté de médecine et des sciences de la santé, Université de Sherbrooke, Direction de la santé publique de la Montérégie, Agence de la santé et des services sociaux de la Montérégie.
answer At the Canadian level, the main independent expert group issuing guidelines on prevention in clinical practice is the Canadian Task Force on Preventive Health Care (CTFPHC) Since 1979, this independent, government-funded, expert group studies the evidence in the literature regarding the main preventive interventions and issues guidelines for clinicians. Their guidelines are available online. (Click hereto view them). The American equivalent of this group is the U.S. Preventive Services Task Force. Their guidelines are also available online. (Click here to view them).
ANSWER CTFPHC Recommendation Grades (for illustrative purposes) No new recommendations were issued between 2006 and 2011. Canadian recommendation classification until 2006 Canadian recommendation classification since 2011: G.R.A.D.E. Recommendations are graded as either strong or weak according to quality of evidence (high quality, moderate quality, low quality) Click here to find out more
answer To find out more, here are a few references* … … on prevention in adults (click on the image): GROULX, S. « La prévention chez l'adulte : une occasion à saisir au vol! », Le Médecin du Québec, vol. 40, no 5, 2005, p. 65-73. L'évaluationmédicalepériodique de l'adulte: Recommandationsadaptées à la pratiquemédicale au Québec, 2014 … on prevention in adolescents (click on the image): LAMBERT, D. « La prévention chez l’adolescent: comment l’aborder? », Le Médecin du Québec, vol. 40, no 5, 2005, p. 55-62. *Please note that these references are available in French only.
Question For this patient, what type of prevention in clinical practice is recommended in terms of counseling?
ANSWER Tobacco Recommendation A (CTFPHC, 1994). More recently, the following interventions have been shown to be effective (CAN-ADAPPT, 2011) : Identify and update patients’ tobacco use status If the smoker is ready to quit, encourage them through counseling and medical treatment; If the smoker is not ready to quit, use the motivational approach to increase the smoker’s chances of quitting; Facilitate access to more intensive counseling (individual, group or by phone) – the more frequent and extended it is, the better the results; Organize your clinic to offer a more systematic approach – such as a call back system, referral procedures for resources in counseling and educational materials. 1 2 3 4 5 CAN-ADAPTT. (2011), "Lignes directrices canadiennes de pratique clinique sur le renoncement au tabagisme : énoncés sommaires." Toronto, Canada.. RetrievedJanuary 2014 fromhttp://www.peelregion.ca/health/professionals/events/pdf/2013/canadaptt-summary-statements.pdf
ANSWER Exercise/sedentary living • Nutritional and exercise counseling for adults without hypertension, diabetes, hyperlipidemia or heart disease • Recommendation C (USPSTF, 2012) Diet (intake of fruit and vegetables) • Recommendations from Canada’s Food Guide (2011) (Click on the image for more information) • Behavioral counseling to promote a healthy diet and exercise to prevent cardiovascular disease • Recommendation C (USPSTF, 2012) Click here to find out more Click here to find out more
ANSWER In conclusion, according to Ms. Sweet Tooth’s characteristics, you can gather that there is stronger evidence supporting the benefits of smoking cessation counseling than of diet and exercise counseling. The former would hence be a priority for her.
Question How would you go about providing good counseling to Ms. Sweet Tooth?
ANSWER • We can use the CTFPHC’s 5 “A” method Click here to find out more
ANSWER At the "Assess" step, it is useful to assess the stage of change according to Prochaska and DiClemente to evaluate the patient’s receptiveness to our advice and readiness to adopt a behavioural change. You will find Prochaska and DiClemente’s 6 Stages of Change on the next slide.
ANSWER Click here to find out more “Changing Behaviour”. AFMC Primer on Population Health, The Association of Faculties of Medicine of Canada, RetrievedJanuary 2014 from: http://phprimer.afmc.ca/Part3-PracticeImprovingHealth/Chapter8IllnessPreventionAndHealthPromotion/Changingbehaviour
Background information (continued) You then decide to ask Ms. Sweet Tooth about her motivation to quit smoking. She tells you that she has no intention of quitting in the next year. She smokes outside the house and never smokes in the car. You consider the pros and cons of her tobacco use.
Question At what stage of change is she according to Prochaska and DiClemente?
answer Ms. Sweet Tooth is at the: Precontemplation stage as she does not intend to stop smoking in the next year. However, for exposure to second hand smoke, she is at the action or maintenance stage.