Download
1 / 9
90 likes | 366 Views
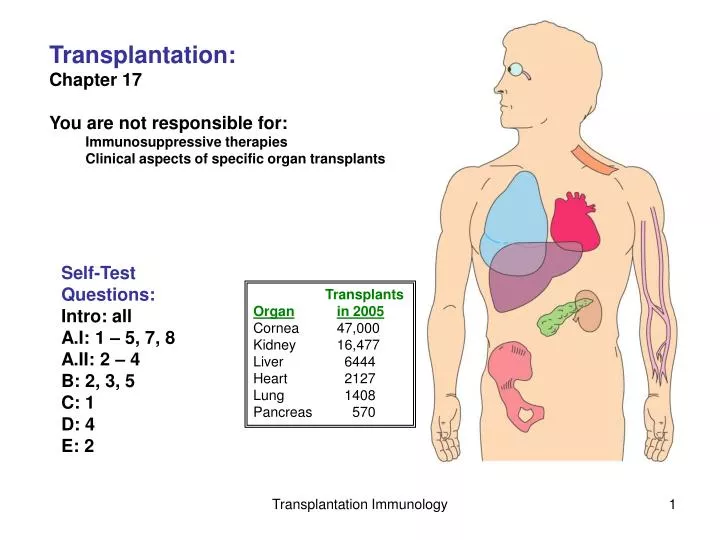
Transplantation: Chapter 17 You are not responsible for: Immunosuppressive therapies Clinical aspects of specific organ transplants. Self-Test Questions: Intro: all A.I: 1 – 5, 7, 8 A.II: 2 – 4 B: 2, 3, 5 C: 1 D: 4 E: 2. Transplants Organ in 2005 Cornea 47,000

E N D
Transplantation: Chapter 17 You are not responsible for: Immunosuppressive therapies Clinical aspects of specific organ transplants Self-Test Questions: Intro: all A.I: 1 – 5, 7, 8 A.II: 2 – 4 B: 2, 3, 5 C: 1 D: 4 E: 2 Transplants Organin 2005 Cornea 47,000 Kidney 16,477 Liver 6444 Heart 2127 Lung 1408 Pancreas 570 Transplantation Immunology
What are different types of tissue transplants? Sources -- Living donor; & self -- Cadaver -- Animal Autologous graft -- e.g., skin, artery transplants -- not rejected Isograft -- e.g., any organ -- not rejected Allograft -- kidney, liver, heart transplants -- rejected; unless Im privileged Xenograft -- rejected, unless non-antigenic -- e.g., heart valves Transplantation Immunology
What are types of rejection? 1. Host-vs-Graft Hyperacute rejection -- rapid: minutes to hours -- humoral; existing Abs; complement -- blood type -- xenografts Acute rejection -- humoral or cell mediated -- days/weeks Chronic rejection -- months / years -- despite immunosuppressive therapy Long term not much improved -- Kidney: half-life only 8-10 years 2. Graft-vs-Host (discussed later) Recipient Abs, attack donor cells Recipient CTLs attack donor cells Recipient Abs against donor MHC 5 Year survival rate (2009) Kidney: 69.3% Heart: 74.9% Liver: 73.8% Lung: 54.4% Transplantation Immunology
What are the mechanisms of Immune rejection Direct vs Indirect allo-recognition Effector cells Rejection mechanisms Transplantation Immunology
What causes ‘Direct’ allo-recognition? Recipient T-cells are activated by: Graft-MHC + Graft peptides Why would T-cells bind to peptides in non-self MHC? Graft-MHC + peptide can resemble Self-MHC + foreign peptide Remember -- MHC polymorphism -- TCR low affinity binding MHC + peptide Transplantation Immunology
What causes ‘Indirect’ allo-recognition? Recipient T-cells are activated by recipient MHC + graft (MHC) peptides Recipient DCs migrate into graft and phagocytose Ags -- MHC peptides -- Minor Histocompatibility Antigens -- polymorphic genes -- Y chromosome-borne genes DCs contribute to: -- humoral activation -- chronic rejection Transplantation Immunology
When does Graft vs Host Disease (GvHD) occur? -- bone marrow -- some solid organ Immune cells of graft react against recipient tissues -- Allo-reactive antibodies -- Cell-mediated attack Occurs in 75%+ of bone marrow transplants But has beneficial effect against leukemic and cancerous cells Transplantation Immunology
How is tissue-matching performed? -- minimizes HLA incompatibility 1. Serological typing -- Abs against specific HLA 2. DNA analysis -- look for HLA-allele specific sequences But how to test against all the different types of HLA antigens?? -- Don’t! HLA typing at NY Blood Center Serology HLA Class I (A,B,C) HLA Class I HLA-B27 DNA analysis PCR- broad allele class resolutionHLA Class I (A,B,C) DNA sequencing allele level resolution, HLA Class I (A,B,C) by HLA-Class II (DRB1)HLA-Class II (DQB1) http://www.nybloodcenter.org/HLA-Typing.do?sid0=92&page_id=185 Transplantation Immunology
Not all HLA genes are equally important Why? In Kidney -- Little MHC-II expressed 6 HLA antigens examined: -- HLA-A, HLA-B, and HLA-DR e.g., HLA-A1 & A2, B7 & B8, DR2 & DR3 Liver-- little MHC-I or -II expressed -- usually only ABO matched What about… Cornea:No matching …Why? Heart:No matching …Why? Increased HLA matching yields only minor improvements in kidney survival Transplantation Immunology