Download
1 / 48
510 likes | 892 Views
Pathophysiology & Management of Acid Base and Common Electrolyte Imbalance in Critically ill. Dr. Shalini Saini. University College of Medical Sciences & GTB Hospital, Delhi. Acid Base Equilibrium. ?. Buffers?. Fixed Cation?. Base Excess/ Deficit?. Anion Gap?.

E N D
Pathophysiology & Management of Acid Base and Common Electrolyte Imbalance in Critically ill Dr. Shalini Saini University College of Medical Sciences & GTB Hospital, Delhi
Acid Base Equilibrium ? Buffers? Fixed Cation? Base Excess/ Deficit? Anion Gap? What is Acid Base Equilibrium About?
Acid Base Equilibrium 50 - 100 mEq/d 12500 mEq/d H+ load from AA metabolism CO2 from metabolism H+ ion Failure of Kidneys to Excrete PO 4--, SO 4-- Ingestion of NH4Cl, CaCl2 Diabetic KA Strenuous Exercise Lactic Acid Acid Base Equilibrium is all about Maintenance of H+ ion concentration of the ECF. Source of H+ ion in Body:
Some Basic Chemistry Definitions: Arrhenius(1903): • Acid: H+ Donor in Solution • Base: OH- Donor in Solution Browsted and Lowry(1923): • Acid: Proton Donor • Base: Proton Acceptor
Some Basic Chemistry pH (Potenz or Power of Hydrogen): Sorenson Negative logarithm of H+ ion concentration to the base of 10 Why pH? Normal H+ ion conc: 0.00004meq/L or 40nEq/L or 4x10-9 mol/L pH converts decimal numbers & takes away negative sign. Normal pH: 7.35-7.45 Normal H+ Conc: 0.00002mEq/L – 0.0001 mEq/L
Acid Base Equilibrium: Solutions: When substances are added to water, 3 simple rules have to be satisfied at all time: • Electrical Neutrality • Mass conservation • Dissociation Equilibrium
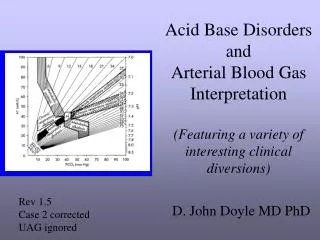
Clinical Concepts: Base Excess: Amount of Acid or Alkali required to return plasma in vitro to normal pH under standard conditions( pH 7.4, PCO2 40 , temp 37 C) Standard BE: BE calculated for Anemic Blood (Hb = 6gm%). • Since Hb effectively buffers plasma & ECF to a large extent. • Quantity of Acid or Alkali required to return plasma in-vivo to a normal pH under standard conditions
Siggard Anderson Normogram To calculate Base Excess
Acid Base Equilibrium: The Henderson-Hasselbalch Equation: H2 CO3 <====> H+ + HCO3- => Ka = [H+ ][HCO3 ]/H2 CO3 Taking Logarithm on both sides & Rearranging: • pH= pKa + log10[HCO3-]/SX*PCO2 pKa = 6.1, S = 0.03(solubility coefficient), PCO2 = 40, HCO3 =25 On putting values & solving, pH = 7.4 Significance: • Includes components of both Metabolic & Respiratory Acid base disorders • Value of any one variable can be determined if other two known. Mostly HCO3- is calculated • pH determined by ratio of [HCO3-]/PCO2 • Increase=> alkalosis, Decrease => Acidosis
Anion Gap: • Estimate of relative abundance of unmeasured anions • Footprint of metabolic acidosis • UC & UA in electrochemical balance equation: Na + UC = (Cl + HCO 3 ) + UA Rearranging equation : UA-UC (AG) = [Na+] - {[HCO3-] + [Cl-]} • Normal Value: 8-12mEq/L • ↑ AG reflects ↑ Unmeasured Anion • Unmeasured Anions- Albumin,Phosphate, Sulphate, Organic acid. • 1mg/dl fall in Albumin, AG↓ by 3meq/l • High AG acidosis- Ketones, Lactate, Methanol. • Normal AG acidosis- Diarrhea.
Clinical Concepts: Acid Base Equilibrium: • Elimination of Acid • Recovery/Regeneration of Base Mechanisms that keep pH stable • Buffering • Compensation • Correction
Clinical Concepts: Buffers: Definition: A substance that can bind or release H+ ions in solution, thus keeping the pH of the solution relatively constant despite addition of large amounts of acid or base. For Buffer HA, HA <====>H+ + A- pH = pKa + log [A-]/[HA] • When [A-] = [HA], pH= pK, buffering capacity is maximum.
Clinical Concepts: Most buffers are weak acids (H+ buffer) & their Na+ Salts (Na+ buffer) • Strong Acids Buffered by Na+ Buffer • HCl + Na Buffer <====> H+ + Cl- +Na+ + Buffer <====> H Buffer + NaCl • Strong Bases Buffered by H+ buffer • NaOH + H Buffer <====> Na+ + OH- + H+ + Buffer <====> Na Buffer + H2O Buffer Effectiveness Depends on: • Quanitity • H2CO3/HCO3- - Most important Extracellular Buffer • Protein Buffers – Most important Intracellular Buffer • pKa – Buffering capacity maximum when pH=pKa
Clinical Concepts: Buffers in ECF: • Carbonate-Bicarbonate Buffer 53% • Plasma (35%) • Erythrocyte(18%) • Hemoglobin 35% • Plasma Proteins 7% • Organic & Inorganic Phosphates 5% Buffers in ICF: • Intracellular Proteins • H2PO4-HPO4- system Intracellular buffers are responsible for ~85% buffering in Met. Acidosis and ~35% in Met Alkalosis and almost complete buffering in Respiratory Acidosis and Alkalosis.
Clinical Concepts: Bicarbonate Buffer: • HCl + NaHCO3-<==>NaCl+ H2CO3<==>NaCl + H2O + CO2 • Useful only for Metabolic Acidosis Hb System: • Both Respiratory & Metabolic Acidosis in ECF
Hemoglobin buffer Chloride Shift Buffers H+ directly HCO3- diffuses out Cl diffuses in
Clinical Concepts: Protein Buffer: • Predominant Intracellular Buffer – Large total concentration • pK = 7.4 • AA have Acidic & Basic Free radicals .COOH + OH- <====> COO- + H2O .NH3OH + H+ <====> NH3 + H2O Phosphate Buffer: • pK = 6.8 • Predominantly Intracellular • Also in renal tubular HCl + Na2HPO4 <====> NaH2PO4 + NaCl NaOH + NaH2PO4 <====> Na2HPO4 + H2O
Clinical Concepts: Compensation: Pulmonary Compensation H+ + HCO3-<====> H2CO3<====>CO2 + H2O • H+ acts on medullary centres. • Metabolic Acidosis – Increased Ventilation • Metabolic Alkalosis – Depression of Ventilation • Minute ventilation increases 1-4l/min for every 1mmHg increase in PaCO2
Clinical Concepts: Renal Compensation: Mechanisms: • Reabsorption of filtered HCO 3- (4000-5000 mEq/d) • Generation of fresh bicarbonate • Formation of titrable acid – (1mEq/Kg/d) • Excretion of NH4+ in urine
MAJOR RENAL MECHANISMS RESPONSIBLE FOR H+ EXCRETION/HCO3- RETENTION RENAL TUBULAR CELL PERITUBULAR BLOOD GLOMULAR FILTRATE Glutamine HCO3- + H+ CO2 HCO3- + H+ HCO3- + H+ HCO3- Na+ HPO42- Na+ NH3 Na+ H2CO3 CO2 + H2 O 1. NaHCO3 CO2 H2PO4- 2. NaHCO3 CA NH4+ 3. NaHCO3 H2O H2PO4- NH4+ CO2 can be obtained from blood or the tubular fluid
Acidemia or Acidosis? • Alkalemia or Alkalosis? Any condition that disturbs acid -base balance by increasing H+ through endogenous production,↓ buffering capaity, ↓ excretion, or exogenous addition is termed as ACIDOSIS Any condition that ↓ H+ is termed as ALKALOSIS Acidemiaor Alkalemia refer to net imbalance of H+ in blood.
Prediction of Compensatory Responses on Simple Acid Base Disorders
pH General approach to acid-base disorder Acidemia pH <7.35 Normal pH7.35-7.45 Alkalemia pH> 7.45 Normal or mixed disorder ↓HCO3 ↑PaCO2 ↑HCO3 ↓PaCO2 Metabolic acidosis Respiratory acidosis Metabolic alkalosis Respiratory alkalosis
Diagnosis of acid base disturbance • Step -1: Is there an acid – base disturbance? look at PaCO 2 & HCO3, whether in normal range. If normal range, noacid-base disturbance or rule out mixed disorder. If abnormal, proceed to step 2. • Step-2: Is there acidemia or alkalemia? • Step-3: What is primary acid base disorder? • Step-4: Calculate the expected compensation? Determine whether actual value matches with the expected compensation. Matching of both confirms diagnosis of primary disorder.
Step 5: Determine the presence of mixed acid-base • Check the direction of changes- As per ‘Rule of same direction’, in simple acid-base disorder PaCO2 & HCO3 changes from normal in same direction. If changes occur in opposite direction; mixed disorder. • If expected compensation > or < than calculated compensation; mixed. • Check for anion gap : • If high AG, High AG metabolic acidosis. • If normal AG , Non-AG metabolic acidosis.
Case scenario: A 66 year old man seen in emergency room. He has had 8 days of severe diarrhea, abdominal pain, & decreased intake, but adequate intake of liquids. His medical history is significant for diabetes & hypertension. Presently on enalapril, aspirin, atenolol, metformin. Physical examination: B.P 105/70, Pulse 72/min, R.R 32. Lab report: Na 136, K 3.9, Cl 114, HCO3 13, creatinine 1.2, glucose 128 Urine: pH 6, Na 32, K 21, Cl 80 ABG: pH 7.27, PO2 90, PCO2 30 • Which acid base disorder is present?
pH low & ↓ HCO3 Metabolic acidosis. • Respiratory compensation : Expected PCO2 = 1.5 X 13 + 8 = 27.5 (Adequate) • Anion Gap = 136– (114 + 13) = 9 (Normal) Non-AG Metabolic Acidosis
Metabolic acidosis • Characterized by fall in plasma HCO3 & fall in pH • Causes:
Clinical manifestations: • Pulmonary changes- Kussmaul’s breathing( deep,regular,sighing respiration) • Cardiovascular changes- if severe (pH<7.2), ↑ susceptibility for cardiac arryhthmias, ↓ response to ionotropes & secondary hypotension. • Neurological changes- headache, confusion to coma. • Other- Renal failure • Diagnosis: • ABG values - ↓ HCO3 , ↓ pH, compensatory ↓ PaCO2
Treatment of Metabolic Acidosis: • Specific management of underlying disorder As a rule treat underlying disorder meticulously. It may be the only required treatment for mild to moderate acidosis & Non-AG acidosis. • Alkali therapy Reserved only for selective patients with Severe Acidemia (controversial) & for Non-AG Acidosis Indications: pH<7.2 with sign of shock or myocardial irritability. HCO3 < 4meq/l Severe Hyperchloremicacidemia Goal: To return pH to about 7.2 & HCO3 ↑ by 8-10meq/l. Amount of HCO3 required= (Desired HCO3 – Actual HCO3 ) X0.3 X Bodywt. Half of the correction is given f/b repeat ABG after sometime.
Case scenario: ABG of a patient with CHF on frusemide pH 7.48, HCO3 34 mEq/l, PaCO2 48 mmHg • pH = alkalosis • HCO3 = s/o metabolic alkalosis • PaCO2 = s/o compensation • Rise in PaCO2 = 0.75 x rise in HCO3 = 0.75 x (34-24) = 7.5 Expected compensation = 40+7.5= 47.5 mmHg ~ actual PaCO2 s/o simple acid base disorder So patient has primary metabolic alkalosis due to diuretics
Metabolic alkalosis • Characterized by ↑ HCO3 , ↑ pH,& compensatory ↑ in PaCO2 • Occurs when there is excess of buffers present, raising systemic pH. • Clinical features: • CNS- ↑ neuromuscular excitability leading to paresthesia, headache. • CVS- hypotension & arrythmias • Others- weakness, muscle cramps
Causes: Metabolic alkalosis by chloride handling • Diagnosis: • ↑ HCO3 ,pH, compensatory ↑ PaCO2 • Serum potassium & chloride low • Urinary chloride estimation useful for diagnosis
Treatment: • Chloride sensitive- IV normal saline volume expansion Discontinue diuretics if possible H2 blockers & PPI in case of nasogastric suction & vomiting • Chloride resistant- Remove offending agent Replace potassium if deficit • Extreme Alkalosis Hemodialysis HCl can also be used(Dose = ∆ HCO3 X wt. X 0.5) ( infused at 0.1mmol/kg/hr)
Case scenario: Following sleeping pill ingestion, patient presented in drowsy state with sluggish respiration with rate of 4/min pH 7.1, HCO3 28 mEq/l, PaCO2 80 mmHg, PaO2 42 mmHg • pH = acidosis • PaCO2 = s/o respiratory acidosis • PaO2 = moderate hypoxemia • HCO3 = s/o compensation • Rise in HCO3 = 0.1 x rise in PaCO2 = 0.1 x (80-40) = 4 mEq/l Expected compensation = 28 mEq/l ~ actual PaCO2 s/o simple acid base disorder So patient has primary respiratory acidosis due to respiratory failure, due to sleeping pills
Respiratory Acidosis • Characterised by ↑ PaCO2 , ↓ pH, & compensatory ↑ HCO3 • Causes: • Airway obstruction- Foreign body,Aspiration, Obstructive sleep apnea, Laryngospasm or Brochospasm. • Neuromuscular disorders of respiration- Myasthenia gravis, Guillain-Barre syndrome, Tetanus, Botulism, Hypokalemia, Cervical spine injury, Obesity • Central respiratiory depression- Drugs(Opiates, sedatives),Brain trauma • Respiratory disorder- Severe Pulmonary edema, Asthma, ARDS, COPD, Pulmonary fibrosis.
Clinical presentation: Headache, confusion, irritability, delirium Severity relates with the rapidity of development of disturbance. • Treatment: • General measures 1. Major goal is to identify & treat underlying cause. 2. Establish patent airway & restore oxygenation. 3. If patient with chronic hypercapnia develops sudden ↑ PaCO2 , search for aggravating factor, vigrous treatment of pulmonary infection, brochodilator therapy, removal of secretions. • Oxygen therapy 1. In Acute , major threat is hypoxia, so oxygen is supplemented. 2. In Chronic hypercapnia, oxygen therapy instituted carefully & in lowest possible concentration.
Mechanical Ventilatory Support 1. Patient selection: In acute acidosis, early use of ventilatory assistance advised. In chronic, a more conservative approach is advisable because of great difficulty in weaning. 2. Indications: • Unstable,symptomatic or progressively hypercapneic. • If signs of muscle fatigue • Refractory severe hypoxemia • Depression of respiratory centre 3. Rate of correction PaCO2 should be gradual & target is usually patient’s prior stable level & in acute should be normal level. • Alkali Therapy Avoid except in severe acidemia or severe bronchospasm.
CASE SCENARIO A 15 year old boy brought from examination hall in apprehensive state with complain of tightness in chest. pH 7.54, PCO 2 21, HCO 3 21 • pH ↑ = s/o alkalosis • ↓ PCO 2 = s/o respiratory alkalosis • ↓ HCO 3 = s/o compensation • expected compensation = 0.2 X (40- 21) = 3.8 • expected HCO 3 = 24-3.8= 20.2 meq/l ~ actual HCO 3 s/o simple acid-base disorder. so, the patient has primary respiratory alkalosis due to anxiety.
Respiratory Alkalosis • Characterised by ↓ PaCO2 due to hyperventilation & leads to ↑ pH. • Diagnosis: ↓ PaCO2 (<35mmHg), ↑ pH , compensatory ↓ HCO3 serum HCO3 does not fall below 15meq/l unless metabolic acidosis is present. • Causes: 1. Hypoxemia- Pulmonary disease( Pneumonia, Fibrosis, Edema,Emboli), CHF, Hypotension, Severe anemia, High altitude. 2. Direct stimulation of respiratory centre- Psychogenic or voluntray hyperventilation, Pain, Hepatic failure, Neurological disorder. • Clinical features: Headache, arrythmias, tetany, seizures. Severity of hypocapnia constitutes grave prognosis.
Treatment • Vigrous treatment of the underlying cause • Mild alkalosis with few symptoms needs no treatment. • As hypoxemia is common cause, oxygen supplememtation is essential.
Case scenario Known case of COPD develops severe vomiting pH 7.4, HCO3 36meq/l, PCO2 60mmHg • pH normal = s/o either no acid –base disorder or mixed • ↑ PCO2 = s/o respiratory acidosis ( due to COPD) • ↑ HCO3 = s/o metabolc alkalosis ( due to vomiting) the patient has mixed disorder , respiratory acidosis & metabolic alkalosis. Normal pH can be due to end result of opposite changes caused by primary disorder.
Mixed Acid Base Disorders • Difficult to diagnose • Suspected whenever pH is normal or if apparent compensation is not adequate in a patient with known primary acid-base disorder. • Mixed metabolic & respiratory acidosis occurs when respiratory compensation is insufficient . • Gram- negative sepsis is a common cause of respiratory alkalosis & metabolic acidosis .
Summary: Acid Base Homeostasis is all about maintenance of normal H+ concentration. Changes in acid base status of ECF have profound and often unpredicatable clinical and laboratory effects, more so during anaesthesia. pH scale is a negative logarithmic scale. Anion gap must always be calculated to decipher more accurately the complex acid-base disorders in critically ill patients. Bicarbonate therapy must be used with caution in view of it’s various deleterious effects.
References Miller’s Anesthesia, 7th Edition Civetta, Taylor, Kirby; Critical care 4th Edition Wylie And Churchill Davidson’s A Practice of Anaesthsia, 5th Edition Morgan Michael , 4th Edition Clinical Application of Blood Gases, Shapiro, 5th Edition Harrison’s Principles of Internal Medicine, 16th Edition