Download
1 / 25
250 likes | 379 Views
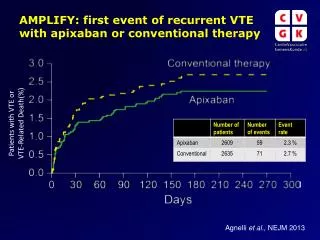
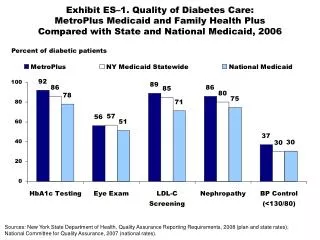
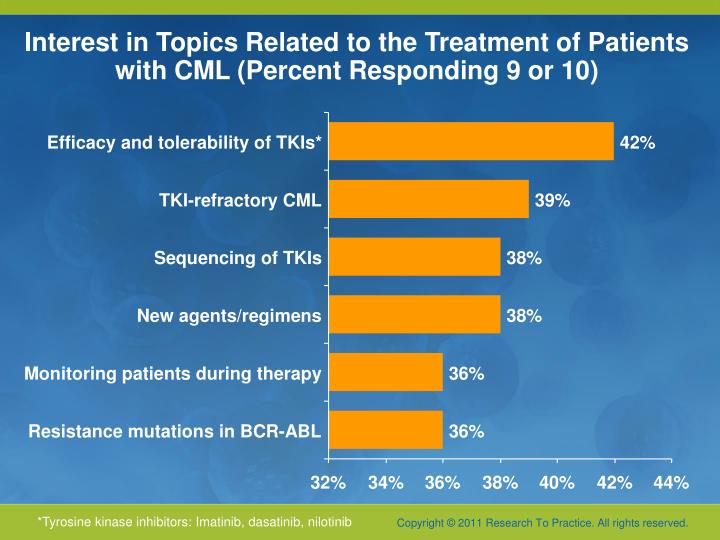
Interest in Topics Related to the Treatment of Patients with CML (Percent Responding 9 or 10). Efficacy and tolerability of TKIs*. 42%. TKI-refractory CML. 39%. Sequencing of TKIs. 38%. New agents/regimens. 38%. Monitoring patients during therapy. 36%. Resistance mutations in BCR-ABL.

E N D
Interest in Topics Related to the Treatment of Patients with CML (Percent Responding 9 or 10) Efficacy and tolerability of TKIs* 42% TKI-refractory CML 39% Sequencing of TKIs 38% New agents/regimens 38% Monitoring patients during therapy 36% Resistance mutations in BCR-ABL 36% 32% 34% 36% 38% 40% 42% 44% *Tyrosine kinase inhibitors: Imatinib, dasatinib, nilotinib
Chronic Myeloid Leukemia (CML) Susan M O’Brien, MD
IRIS 8-Year Update: Outcome After Imatinib 37% Deininger M et al; Blood 2009;114(22):462.
Nilotinib vs Imatinib in Newly Dx CML (ENESTnd) R A N DOMI Z ED * Nilotinib 300 mg BID (n = 282) • N = 846 • 217 centers • 35 countries Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283) Follow-up 5 years • Primary endpoint: MMR at 12 months • Key secondary endpoint: Durable MMR at 24 months • Other endpoints: CCyR by 12 months, time to MMR and CCyR, EFS, PFS, time to AP/BC on study treatment, OS including follow-up *Stratification by Sokal risk score Hughes et al. ASH 2010; abst #207
Nilotinib vs Imatinib in Newly Dx CML-CP (ENESTnd). Primary Endpoint - MMR Rate at 12 Months (ITT Population) P < .0001 P < .0001 Patients with MMR (%) Larson RA et al. JClin Oncol 2010;28; Abstract 6501. Saglio G et al. N Engl J Med 2010;362; Abstract 2251.
IRIS 8-Year Results: Annual Rate of Events on Imatinib AP/BC • EFS = 81% • Freedom from progression to AP/BC = 92% • 1 progression to AP/BC and 2 non-CML related deaths in year 8 Deininger et al. ASH 2009. Abs # 1126.
Dasatinib 100 mg QD (n = 259) Imatinib 400 mg QD (n = 260) Dasatinib versus Imatinib Study in Treatment-Naïve CML: DASISION (CA180-056) Study Design • Primary endpoint: Confirmed CCyR by 12 months • Secondary/other endpoints: Rates of CCyR and MMR; times to confirmed CCyR, CCyR and MMR; time in confirmed CCyR and CCyR; PFS; overall survival • N = 519 • 108 centers • 26 countries Follow-up 5 years Randomized* *Stratified by Hasford risk score Shah et al. ASH 2010; abst #206.
DASISION: First-Line Dasatinib vs Imatinib in CML-CP CCyR Rate by 12 Months (ITT) P = 0.0011 P = 0.0067 CCyR (%) CCyRby 12 months Confirmed CCyRby 12 months Kantarjian. N Engl J Med 362: 2260, 2010.
DASISION: Progression to AP-BP (ITT) 100 n/N6/259 9/260 • No patient who achieved MMR progressed to AP/BP CML • 5 patients who achieved a CCyR progressed to AP/BP CML (2 dasatinib, 3 imatinib) • Rates of progression-free survival at 18 mos: 94.9% for dasatinib and 93.7% for imatinib Shah N et al. Blood 2010;116: Abstract 206.
DASISION: Confirmed CCyR (ITT) P = 0.0366 P = 0.0086 Shah N et al. Blood 2010;116: Abstract 206.
Definitions of PFS-EFS in CML Kantarjian et al. Blood 2010:116; Abst #672.
Outcome According to Different Definitions of EFS/PFS - Because EFS and PFS are important in determining whether new TKIs are better than imatinib in front-line therapy, precise and common definitions of these endpoints are needed. Kantarjian et al. Blood 2010:116;Abst #672.
Data cut-off: 20Aug2010Hughes TP, et al. ASH 2010. Abstract 207.
Data cut-off: 20Aug2010Hughes TP, et al. ASH 2010. Abstract 207.
Data cut-off: 20Aug2010Hughes TP, et al. ASH 2010. Abstract 207.
Data cut-off: 20Aug2010Hughes TP, et al. ASH 2010. Abstract 207.
Data cut-off: 20Aug2010Hughes TP, et al. ASH 2010. Abstract 207.
100 DASISION: Grade 3/4 Cytopenia • Grade 3/4 bleeding occurred in 2 patients on dasatinib and 3 patients on imatinib • 6 patients on dasatinib and 3 patients on imatinib D/C Rx due to cytopenia Shah N et al. Blood 2010;116: Abstract 206.
Common Nonhematologic Drug-Related AEs (≥10%) *Includes 11 MedDRA preferred terms † Includes myalgia, muscle inflammation and musculoskeletal pain
What Clinicians Want to KnowA Live CME Event Addressing the Most Common Questions and Controversies in the Current Clinical Management of Select Hematologic CancersSunday, June 5, 20117:00 PM – 9:30 PMChicago, Illinois Moderator Neil Love, MD Faculty Sergio Giralt, MDJohn P Leonard, MD Lauren C Pinter-Brown, MD Antonio Palumbo, MDSusan M O’Brien, MDProfessor Michael Hallek
What is your preferred initial systemic treatment for chronic-phase CML?
Have you discontinued imatinib, dasatinib or nilotinib for patients responding with sustained molecular CR?
What Clinicians Want to KnowA Live CME Event Addressing the Most Common Questions and Controversies in the Current Clinical Management of Select Hematologic CancersSunday, June 5, 20117:00 PM – 9:30 PMChicago, Illinois Moderator Neil Love, MD Faculty Sergio Giralt, MDJohn P Leonard, MD Lauren C Pinter-Brown, MD Antonio Palumbo, MDSusan M O’Brien, MDProfessor Michael Hallek