Download
1 / 61
640 likes | 666 Views
Malignant Melanoma. Tommy Busick, MD Resident’s Conference November 2, 2004. Melanoma Rising Incidence. Lifetime risk in 1979 1:250 Today 1:64

E N D
Malignant Melanoma Tommy Busick, MD Resident’s Conference November 2, 2004
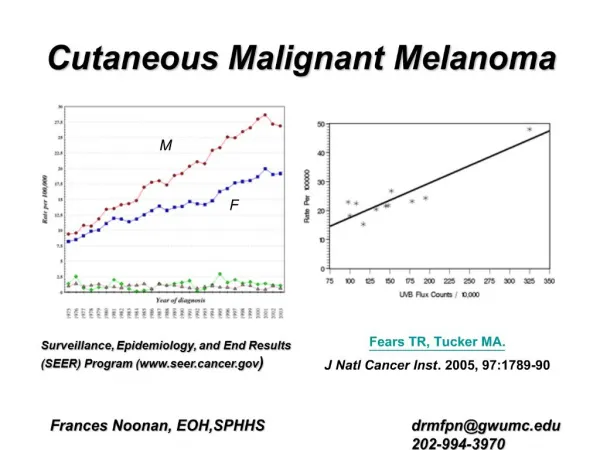
Melanoma Rising Incidence • Lifetime risk in 1979 1:250 Today 1:64 • Rank among cancers in 1979 Women 10th Men 11th Today Women 7th Men 5th • Total incidence 1979 13,600 Today 55,100 • Total deaths in 1979 4,300 Overall survival 75% Today 7,910 Est. survival 90% • Rise in new cases only exceeded by lung CA in women
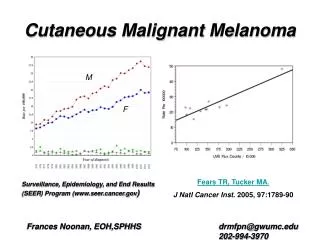
Why the Changes? • Actual increase in the incidence of disease due to increased recreational sun exposure. • Greater public awareness/surveillance so more cancers are found. • Incidence has actually leveled off starting in the 90’s due to this increased awareness. • Cancers are detected earlier, thus the lower mortality rates. Average Breslow depth 1979 2mm Today 1 mm
ABCD’s • A = Asymmetry • B = Border irregularity: a jagged or "coast of Maine" type border represents horizontal extension of malignant cells • C = Color: blue-black, white, red and grey-brown coexist, reflecting the presence of malignant extension • D = Diameter: greater than 6 mm is suspicious for pigment cell atypia • Amelanotic melanomas do occur and can present as rapidly growing flesh-colored or nonpigmented tumors
RF’s for Melanoma: MMRISK • M Moles: atypical/dysplastic (>5) • M Moles: common moles (>50) • R Red hair and freckling • I Inability to tan: skin types I and II • S Sunburn: severe sunburn especially in/before adolescence • K Kindred: family history of melanoma
Sun Exposure and Melanoma (ORs) Exposure Summary result (95% CI) Intermittent 1.87 (1.67–2.09) Occupational 0.76 (0.68–0.86) Total exposure 1.20 (0.00, 1.44) Adult/lifetime sunburn 1.91 (1.69, 2.17) Adolescence sunburn 1.95 (1.60, 2.36) Childhood sunburn 1.62 (1.35, 1.95) Significant positive association for intermittent exposure and positive associations for sunburn in adolescence and sunburn in childhood
Genetics of Melanoma • Approximately 10% of melanomas are familial • Familial Atypical Multiple Mole Melanoma (FAMMM) Syndrome (>50-100 melanocytic nevi and melanoma in at least 1 first degree relative) CDKN2A tumor suppressor down regulates p53 CDK4 oncogene • MC1R - melanocortin 1 receptor • BRAF - gain of function in a protein kinase • HRAS - implicated in acral melanomas
Gender Differences • Males are more likely to get melanoma 19/100,00 than females 14/100,000 • Males most common site is trunk • Females most commonly lower extremity • Both can get melanoma anywhere • Difference most likely related to clothing differences • Studies have shown that intermittent sun exposure on unexposed skin is important in the etiology of melanoma
Ethnicity • Incidence of melanoma among whites is approximately 20 times higher than among blacks • Hispanics in LA have melanoma 2–3 per 100,000 • Whites 11 per 100,000 • For basal cell and squamous cell carcinoma, rates among blacks are 1/80 of the rates among whites
Types of Melanoma • Superficial spreading melanoma • Lentigo maligna melanoma • Melanoma arising in dysplastic nevus • Nodular melanoma • Acral lentiginous melanoma • Nonpigmented/amelanotic • Melanoma of mucous membranes • Desmoplastic (Spindle Cell) Melanoma
Superficial Spreading Melanoma • These lesions tend to exhibit horizontal growth for variable periods prior to vertical growth • 70% of melanomas are of this type
Lentigo Maligna • Broad macular lesion usually on the face of elderly individuals • 5% of melanomas present in this fashion
Dysplastic Nevus • Melanoma can arise from these in congenital lesions but more commonly from nevi acquired later in life
Nodular Melanoma • Nodule or tumor often extending above the surface of the skin • Thought to have an abbreviated radial growth phase and accounts for 15% of all melanomas • Worst prognosis as early metastasis
Acral Lentiginous Melanoma • Lesions are by definition isolated to the distal extremities often occurring in the subungual or periungual regions • Representing 5% of melanomas • Most frequent melanoma in dark skinned individuals
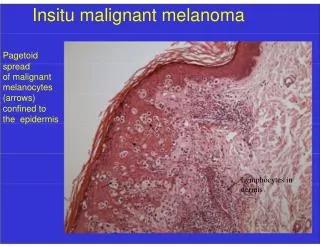
Clark Level • Level of invasion based on cutaneous anatomy. Deeper invasion correlates with worse prognosis, but not as well as Breslow depth. • A. Clark level I: Involvement of the epidermis only. • B. Clark level II: Invasion into but not filling of papillary dermis • C. Clark level III: The papillary dermis is filled with neoplastic cells • D. Clark level IV: Invasion into the reticular dermis • E. Clark level V: Invasion into the subcutaneous fat
Breslow Depth • Vertical distance in mm from the base of the granular layer in the overlying epidermis to the deepest melanoma cell in the subepidermal tissues. • Best prognostic indicator available • TIS In Situ Near 100% Survival • TI <1 mm • T2 1.01-2.0 mm • T3 2.01-4.0 mm • T4 >4 mm 45-63% if node negative
Surgery for Melanoma • Up until the 1970s, margins of excision ranging from 3 to 5 cm were the standard • Current recommendations from 4 randomized prospective trials • 1-cm radial margins for primaries up to 1 mm thick • 2-cm margins for primaries up to 4 mm thick
Excision should include skin and underlying subcutaneous adipose down to the muscle fascia • Excision of the muscle fascia has not been shown to improve disease control • Limited margins of excision reduce the need for skin grafts, complex tissue closures, and ultimately the costs and morbidity of patient care
Likelihood of Recurrence • Primary tumor thickness • Ulceration • Increasing patient age • Anatomic site: head, feet, and hands • Unfortunately, most patients with local recurrences eventually die of distant disease
Elective Lymph Node Dissection • Considered a valuable staging procedure in past • Cost, morbidity, and overall low yield of tumor-containing nodes have led most surgeons to abandon this procedure as a routine part of patient care • Tumor status of the regional lymph nodes has become exceedingly important for determining patient prognosis and directing the use of adjuvant therapy
Sentinel Node Biopsy • Technetium 99m and sulfur colloid • Scintillation camera is used to document the drainage pattern • Isosulfan blue dye injected at the site of the primary melanoma • Handheld gamma probe used to determine the radioactive counts over the blue nodes • Excise “hottest” node • If positive, sentinel complete lymph node dissection
Immunohistochemical Staining • Detect micrometastatic disease in nodes • Specific antibodies to melanoma-associated proteins • S-100, HMB-45, Melan-A, and NKI/C361 • S100 highly sensitive but limited by low specificity • HMB-45 most widely used because higher specificity, but has false negative in 10-15%
Radiation • No great studies on this • Radiotherapy as primary treatment for cutaneous melanoma is rarely indicated • Exception is the case of extensive facial lentigo maligna melanoma • Large tumors difficult to resect • Reasonable tumor control and good to excellent cosmesis
Very few series supporting the routine use of adjuvant local irradiation • In general, indications for adjuvant radiation include head and neck desmoplastic primaries, thick or ulcerated primaries, those with close or positive resection margins, and locally recurrent disease • Despite a lack of randomized clinical trial data, generally recommend adjuvant axillary irradiation when either extracapsular extension is noted histologically, involved lymph nodes are ≥3 cm in size, four or more lymph nodes are involved, or disease is recurrent after initial surgical resection
Metastases • Notorious for late metastasis • Once melanoma has spread to a distant site median survival is 7 to 8 months and 5-year survival is less than 5% • Survival worse with early metastasis and multiple sites • Grim prognosis has remained relatively unchanged for 30 years • Response to conventional chemotherapy is rarely complete • Metastasectomy can improve survival in carefully selected patients as it can rapidly render a patient disease-free • Complex imaging techniques help select these patients with fewer mets • No general recommendations for these surgeries
Survival After Metastsis Site Survival (mos) 2 years 5 years Skin, nodes 15 29±3% 14±2% GI tract 11 28±5% 12±4% Lung 8 12±1% 4±1% Bone 6 9±3% 4±2% Liver 4 6±1% 2±1% Brain 4 8±2% 3±1% All sites 7.5 14±1% 6±1%
Chemotherapy • Chemotherapy in the treatment of melanoma is usually reserved for metastatic disease • Dacarbazine is the most active single-agent with response rate of 20% that last 6 months and only 2% of patients with sustained remission • Cisplatin, nitrosoureas, taxanes, and vinblastine have been tried with response rates of 10-20% and significant toxicity • Combination chemotherapy (CVD most common) has been extensively explored with greater toxicity and no improvement in overall survival
Biochemotherapy • Interferon-alfa alone failed to demonstrate a significant improvement in overall response and survival with increased toxicity • Interleukin-2 also does not seem to improve responses rates or survival • IL-2 may interact synergistically with cisplatin and multiagent regimens with this combination are currently being explored • Chemotherapy in combination with INFa and IL-2 is considered in the classic biochemotherapy regimen
Novel Agents • Temozolomide new alkylating agent • G-3139 (Augmerosin) - BCL-2 antisense protein • PS-341 is a proteasome inhibitor being investigated as a single agent and in combination therapy possibly as a sensitizer to chemo • Epothilone (BMS –277550) is a novel antitubulin chemotherapy • Several other innovative treatment options also under investigation, such as novel vaccines, fusion proteins, and dendrite cell vaccines
Bottom Line • The early diagnosis and surgical treatment of melanoma are the only approaches to date that have increased survival.