Download
1 / 73
740 likes | 987 Views
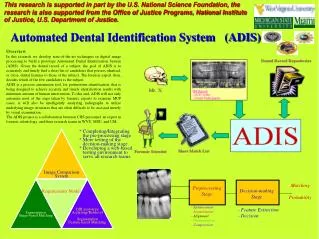
CT for ADIS Module. Rob Stewart September 2012. CT Head. Primary investigation of choice for the detection of acute clinically important brain pathologies • Good for detecting: – Bleeds – Fractures – Base of skull – Infarcts. Effective Doses in CT and Radiographic Examinations.

E N D
CT for ADIS Module Rob Stewart September 2012
CT Head • Primary investigation of choice for the detection of acute clinically important brain pathologies • Good for detecting: – Bleeds – Fractures – Base of skull – Infarcts
Effective Doses in CT and Radiographic Examinations • CT gives rise to approx 50% of the population dose for medical exposures • Manual use of mA should be kept to a minimum - mA modulation
Guidelines Premise • Substituting one for the other will improve patient management • A CT scan is better than a skull x-ray in head injury
Service Effects? Positive • Scanning will show what is going on inside the head rather than just whether the skull is broken • Patients with a negative scan may be allowed home rather than be admitted for observation Negative • There will be a huge increase in the number of CT scans performed • Radiologists: • Lost sleep yet having to work the next day • Currently problems with both having to authorise studies as well as report them • Radiography: • Increase in workload makes on call from home impractical • Time off next day mandatory
Baselines Supra-orbital
Baselines Supra-orbital • Base of skull to superior orbital margin Advantage • Reduced radiation dose to the lens Disadvantages • Increased artefact in the posterior fossa • Unable to assess sinus disease
Baselines Anthropological (Reid’s) Baseline
Baselines Anthropological Baseline • EAM to lower orbital margin Advantages • Good visualisation of the posterior fossa • Ability to assess sinus disease/ pathology in the orbits • Assessment of Chiari malformation – cerebellar tonsil descent Disadvantage • Increases dose to the eyes
Baselines Cerebellar Tonsils Importance of coverage !
Baselines SO Baseline ANTRO Baseline Effects on Temporal Lobe Visualisation
Choice of Baselines Depends on Radiologist Neuro-centre
Radiation Dose To Lens Lens of Eye Dose • “Angling the beam to avoid the orbit decreases dose to the lens by 87% while the severity of beam hardening artefact was not significantly different” • “Only 32% (58 of 184) of sample angle the gantry to avoid the eyes” Yeoman et al, 1992 • “Supraorbital-mental base line should always be used in routine CT brain scanning” McLennan & Hadley, 1995
Radiation Dose To Lens Radioprotection to Eyes During Scanning • Comparison of reduction in CT dose through the use of Bismuth shields • 48% reduction using shield • Artefact in globe but not brainHeaney (2006)
Artefacts • Any discrepancy between reconstructed CT numbers in the image and the true x-ray absorption characteristics of the tissue area which degrade the diagnostic quality of the image • In addition, through inadequate compensation in reconstruction for known effects of x-ray absorption • Some can be corrected by scanner software (reconstruction) • Some corrected by patient positioning and parameter selection is important • Some artefacts pertain to helical scanning only i.e. stair-step, zebra and artefacts in the transverse plane (Hofer, 2007)
How to Look at a CT • Know why you are doing the scan • Is there mass effect present? • Is there any blood? • Look at the periphery of the brain • Look at the bones/ soft tissue in trauma
CT Number Scale (Hounsfield Units) • Grey Levels on CT image represent attenuation in each pixel • Grey levels expressed in Hounsfield Units (HU) • Water = 0 HU • Air = -1000 HU • Bone = 1000 HU
Signs of Mass Effect • Ventricles narrowed/ displaced • Midline shift
Is There Blood Present • In the brain? • In the ventricles? • In the subarachnoid space / cisterns? • In the periphery?
Blood, cells and Serum, Clot • CT appearance of blood depends on only one factor Electron density • Clot is white Exceptions Rapid bleeding Coagulopathy Extreme anaemia • Old haemorrhage has same density as CSF Iron is scavenged
CT Appearance of Blood • Acute 0-7 days –White • Subacute 7-22 days –Same as brain • Chronic 22 days –Dark –White in dark if re-bleed
Is there Pneumocephalus? • Air within skull vault will show up black • Indicative of a fracture to outside • Can be viewed on lung windows
Normal Variants • Calcification • Fat density
Brain- Anatomy Frontal Sinus Sphenoid Sinus Temporal Bone Brainstem Ocular Muscle Cerebellum In Posterior Fossa
BRAIN -Anatomy Frontal Sinus Basilar Artery 4th Ventricle Falix Cerebri Lateral Sulcus Temporal Lobe Mastoids
Brain structure: Meninges of brain • Dura • Arachnoid • Pia
Dura • Tough membrane attached to inner table of the skull • The dura splits to form: –falxcerebribetween the cerebral hemispheres –tentoriumlies above the cerebellum
Arachnoid • A delicate membrane between the • DuraandPia • Attached to the Pia by a network of fibres
Pia • A thin membrane adherent to the brain
Types of bleed into linings • Extradural • Subdural • Subarachnoid
Extra dural • Skull fracture • Laceration of dural artery – Usually middle meningeal • Blood collects between inner table of skull and outer layer of dura • Dura stripped from its firm attachment to inner table • Biconvex mass
Subdural • Acceleration, deceleration and rotation • Tearing of cortical veins as they cross subdural space • Crescent shaped • Varying ages • Can rebleed from vascularised membrane that forms around a chronic subdural –Acute on chronic subdural
Subdural Bleed Bleed
Sub ArachnoidHaemorrhage • Case Study • 47 year old woman • Admitted with severe headache and vomiting to A & E • CT revealed subarachnoid haemorrhage
Sub-Arachnoid Haemorrhage • Bleeding in the sub-arachnoid space of the brain • Between arachnoid membrane and pia mater • Trauma or spontaneous • Non traumatic: • 80% are berry aneurysm • 20% vascular malformations i.e AVM • May lead to death or disability if not treated quickly • Treatment: Close observation, neurosurgical • CT without contrast is the most sensitive study in SAH • The CT findings of SAH may be subtle particularly in the subacute stage. (MRI may help here)
Intracerebral Causative factors : • Stretching and shearing injury • Often -impaction of the brain against the skull on the side opposite to the injury. Thus they may be seen directly opposite the impact site (contrecoup injury). • The inferior frontal lobes and anterior temporal lobes common sites after a blow to the back of the head.
Petechial Haemorrhage – Diffuse Brain Injury • Multiple contusions -visible at the grey/white matter interface. • Shearing injury with rupture of small intracerebral vessels • Imply severe diffuse brain injury with a poor prognosis ? • May not be apparent on a scan performed immediately after the injury. • MRI is more sensitive to diffuse brain injury, particularly in the absence of haemorrhage.
Vault & Base Fractures • Not always visible, but blood in the sinus cavities (i.e. sphenoid sinus) suggests their presence • Important as such patients are prone to developing meningitis and require antibiotic prophylaxis • If the patient has clinical evidence of skull base fracture (i.e. CSF rhinorrhoea or bleeding from the external auditory meatus), clinical findings should override ‘normal’ CT findings.