Download
1 / 14
140 likes | 154 Views
Passenger Emergencies. Guidance for Controllers. Typical M edical P roblems on Board.

E N D
PassengerEmergencies GuidanceforControllers
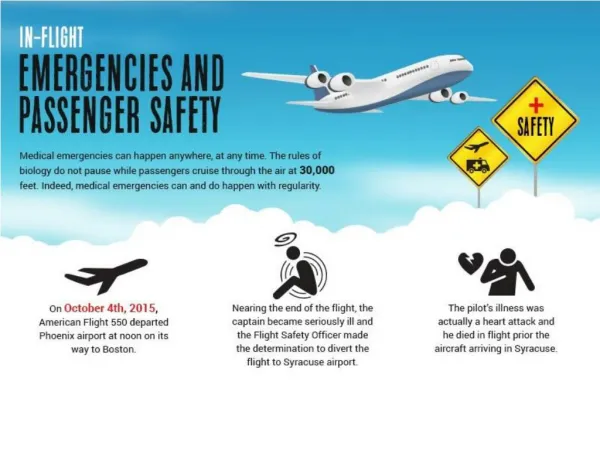
TypicalMedicalProblems on Board Researches show that inflight medical emergencies are rare, occurring at a rate of approximately 15 to 100 per million passengers, with a death rate of 0.1 to 1 per million.On the other hand, if a serious health problem occurs on board, the access to medical care is limited. While there is a plethora of medical issues that can arise during a flight, researches have shown that the most common problems are: Fainting; Heart attack; Dehydration; Nausea / vomiting. Not every medical problem leads to the flight crew declaring a medical emergency. In many cases the flight crew and/or other passengers (e.g. doctors, passengers with medical education and experience) are able to successfully resolve the situation.
Contributing Factors for Passenger Medical Emergencies • The following factors, individually and in combination, can exacerbate a health problem that a person might already have (e.g. heart or lung diseases): • Air travel is a source of stress and anxiety for some people; • Cabin altitude for an airliner in cruise is generally in the range of 6000 to 8000 feet; • Low air humidity and alcohol/caffeine drinks can contribute to dehydration; • People usually sit, with minimal movement, for long periods of time.
Controllers' Actions • The advice given in this section is derived from good practices and common sense and is neither to be considered exhaustive nor intended to replace local procedures. • Generally, the ASSIST (A - acknowledgeS - separateS - silenceI - informS- supportT - time) routine should be followed, bearing in mind the specifics of the situation: • Acknowledge the situation and clarify whether an emergency is being declared; • Obtaining as much information as necessary, e.g. number of sick passengers, the exact nature of the medical problem or, if the medical problem is not determined, the symptoms being manifested plus any other relevant details of the situation. Determine, as necessary, if the passenger illness is recognised as infectious (e.g. symptoms such as constant productive cough and signs of fever); • Clarify the intentions of the flight crew; most likely they will choose to land on the nearest suitable aerodrome; • Assist the flight crew by: • Providing a shorter route to the aerodrome chosen; • Providing information on the aerodrome chosen (if requested); • Giving priority to the aircraft that has declared an emergency (e.g. issuing separation-related instructions to other aircraft); • Coordinate appropriate services on arrival; • Inform the supervisor. Outsourcing some of the workload (e.g. coordination with the aerodrome) could prove useful, especially in heavy traffic situations.
Considerations • Unlike most other emergency situations (e.g. fire on board, engine failure, etc.), there is usually no abrupt peak in cockpit workload at the moment when a passenger medical emergency occurs. Therefore, it is unlikely that questions for clarification of the situation will be considered as harassment. The risk of not obtaining vital information (by avoiding possibly unnecessary questions) is higher than the risk of hindering crew performance (by too much communication). Be aware, however, that one of the pilots may be occupied with communication with a medical support service or with Company operations, and the remaining pilot may elect to defer the questions until those tasks have been completed. • Focus on information quality rather than speed; there is usually sufficient time to obtain correct data and mishearing can lead to drastic consequences (e.g. “two sick passengers” might sound like “two-six passengers”). • If there is/are suspected case(s) of highly contagious disease on board, a system to deal with the emergency situation should be ensured in coordination with the airport authorities as necessary (e.g. outbreak quarantine measures with restricted/controlled access to the aircraft, aircraft parked at isolated stand etc.) to avoid and to reduce the possibility of an infectious disease outbreak.
General • In-flight medical emergencies can be broadly divided into two categories - injury related or health related situations. Injuries can occur as a result of a turbulence encounter, luggage falling from an overhead bin, an onboard altercation or due to burns or scalds resulting from contact with hot liquids or galley ovens. Health issues for a single passenger can range from fainting or shortness of breath to allergic reaction to missed medication to gastrointestinal issues to stroke, heart attack or even death. In very rare cases, food poisoning or a commutable disease may affect an number of passengers at the same time. The article Public Health and Aviation deals with the circumstances of discovery of a commutable disease while enroute and that situation will not be addressed in this article. • When an in-flight medical emergency occurs, immediate access to care is limited. Cabin crew are trained to provide first aid and limited medical assistance but are not qualified to deal with all potential situations. It is, therefore, critical that airlines have protocols in place for actions to be taken in the event of an on-board medical emergency. Adherence to these protocols will help to ensure the best possible outcome for the situation at hand.
Discovery • Cabin crew may become aware of a passenger in medical distress by direct observation. More often, the situation is brought to their attention by the individual, a travelling companion or another nearby passenger. • The first flight attendant at the scene will normally take charge of the patient and alert other cabin crew members who in turn will provide any required assistance inclusive of retrieving any required emergency equipment and advising the Captain of the situation and progressively keeping him/her informed of any changes in patient status.
Flight CrewResponse • Flight crew response to an on board medical emergency will depend on the nature of the problem, the degree of urgency for medical intervention and the location and phase of flight in which the situation occurs. Unless the situation is considered immediately life threatening, it is normal that no decisions will be taken until more information is available through an assessment and diagnosis process. However, the flight crew should use the time between first notification and the end of the assessment/diagnosis process to consider their diversion options and the implications of any diversion decision. Consultation with Company operations may be prudent at this stage.
Assessment • The attending flight attendant will immediately do a preliminary assessment of the patient. If the patient is conscious, the flight attendant will use a question and answer protocol (with the help of an interpreter if required) to determine why the patient is in distress. If the patient is not conscious, the preliminary accesssment will include the A,B,C's of first aid: • Airway (does the patient have an open airway?) • Breathing (is the patient breathing) • Circulation (is there a detectable heartbeat) • If the answer to any of these questions is no, appropriate first aid techniques inclusive of artificial respiration or cardiopulmonary resuscitation (CPR), will be initiated.
On-Board MedicalEquipment • Regulations on what emergency equipment must be carried and what optional equipment can carried vary by National Aviation Authority. In all cases, one or more first aid kits will be on the aircraft. These contain most of the items that might be required to deal with a non life threatening injury such as a burn, cut or broken bone. Cabin crew are fully trained in emergency first aid procedures. • Therapeutic oxygen is also universally carried, normally in portable oxygen cylinders fitted with a regulator and mask. Cabin crew are trained to administer oxygen to passengers experiencing breathing difficulties or are manifesting other symptoms for which supplemental oxygen is appropriate. • An Automated External Defibrillator (AED) is carried on board most commercial aircraft for heart related emergencies. Cabin crew are trained and qualified in the use of this equipment and are also trained and qualified in CPR (cardiopulmonary resuscitation)
A physician's kit or emergency medical kit, containing various drugs and both diagnostic and invasive medical instruments, is carried on board many commercial aircraft. Cabin crew are not trained or qualified to administer drugs and the contents of this kit can only be accessed and administered by a licensed medical practitioner, should one be on board. Typically, a physician's kit will contain some or all of the following (Source: Aerospace Medical Association): • Medications • Epinephrine 1:1,000 • Antihistamine, injectable (inj.) • Dextrose 50%, inj. 50 mL (or equivalent) • Nitroglycerin tablets or spray • Major analgesic, inj. or oral • Sedative anticonvulsant, inj. • Antiemetic, inj. • Bronchial dilator inhaler • Atropine, inj. • Corticosteroid, inj. • Diuretic, inj. • Medication for postpartum bleeding • Normal saline • Acetylsalicylic acid for oral use • Oral beta-blocker • Epinephrine 1:10,000
EquipmentStethoscope • Sphygmomanometer • Airways, oropharyngeal • Syringes • Needles • IV catheters • Antisepticwipes • Gloves • Sharpsdisposalbox • Urinarycatheter • Intravenousfluidsystem • Venoustourniquet • Spongegauze • Tapeadhesive • Surgical mask • Flashlightandbatteries • Thermometer (nonmercury) • Emergencytrachealcatheter • Umbilicalcordclamp • Basic life supportcards • Advanced life supportcards