Download

1 / 53
540 likes | 597 Views
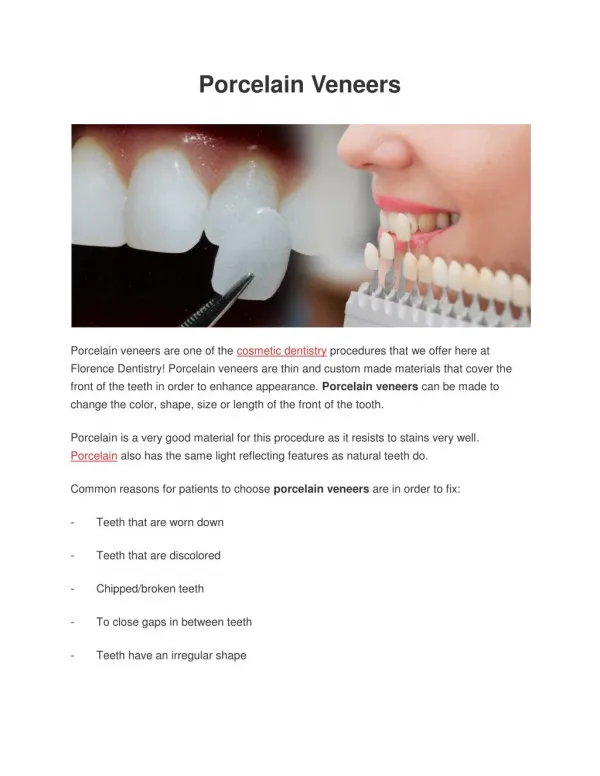
Porcelain veneers are known to be the most effective, long-lasting, and appealing cosmetic procedure to give a professional smile. The various problems like discolored teeth, chipped teeth, rotated teeth, crowded teeth, or gaps can be easily solved by porcelain veneers.The porcelain veneers are extremely natural-looking and can easily cover any staining present on the tooth structure. It is a great option to improve the smile efficiently and at an affordable cost.

E N D
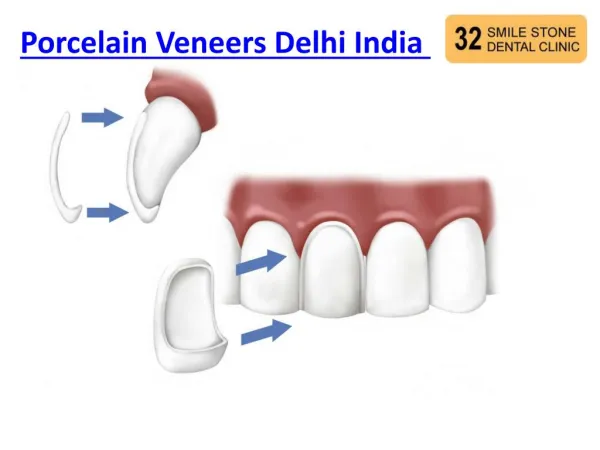
Veneer • Porcelain Laminate veneer
Benefits : • Minimally invasive t/t method. • Shape, position and surface appearance : Change of canine into lateral incisor. Tooth length, Alignment, Eliminating any displasia / distrophy • Colour – Bleaching ineffective. • Durability – Stand up extremely well, Dicor and Empress. • Light transmission – Characteristics of natural enamel, bonding material colour of dentin and not seen as maskin agent, Transmit light progressively. • Tissue response • Speed and simplicity
Disadvantages : • Preparation – no rectification, special instrumentation • Esthetic results – heavy discolouration, monochromatic colour. • Bonding procedures – Error failure, crucial and demanding • Fractures – Prior to bonding, No pressure at Try-in • 90% of fracture – occlusal edge or angle. • Inadequate depth • Cohesive nature • Restrict the flexural stresses • Fracture rate – no incisal coverage
Problems in laboratory : Handling layering or segmental build up – 0.7 to 0.3 mm. Post-firing modification : Feldspathic can not be re-fired IPS empress / Duceram-LFC Temporization Difficult to adjust at margins. Poor marginal integrity Unrealistic long-term expectation Lacks – tensofrictional grip.
New classification of indications for porcelain veneers Type I : Teeth resistant to bleaching Type IA : Tetracycline discoloration of degrees III and IV Type IB : No response to external or internal bleaching Type II : Major morphologic modifications Type II A : Conoid teeth Type II B : Diastemata and interdental triangles to be closed Type II C : Augmentation of incisal length and prominence Type III : Extensive restoration (adults) Type III A : Extensive coronal fracture Type III B : Extensive loss of enamel by erosion and wear Type III C : Generalized congenital and acquired malformations.
Contraindications • Insufficient surface enamel • Pulpless teeth • Unsuitable occlusion • Parafunction • Unsuitable anatomical presentation • Single laminate veneers • Caries and fillings • Poor dental care and hygiene
Case selection : • Static and dynamic occlusal relationship • Mode of failure is fractures • Occlusion will dictate • Contacts • Occlusal interferences and parafunction habits. • Periodontal and oral health status. • Forms a strong foundation • Mouth breathers • Condition of tooth • Degree of discolouration • Bleach • Tetracyclin staining • Veneers appear opaque • Opaque porcelain preferred over GIC
Extent of caries • Little or no enamel • Surface area of enamel if decreased by 50% • Extent of restoration • Small enough • Cavity design • Quality of tooth : • Amount of enamel • Amelogensis imperfecata and dentinogenesis imperfecta. • Patients motivation • Home care and regular recalls • Patient’s expectations • Realistic • Diagnostic wax up • Oral habits • Nail or pencil biting
Advantages : • Less sensitive • Multiple teeth • Longivity • Non invasive Types of veneers Partial veneers Full veneers Direct Indirect • Preferred to be non invasive • Advantages : • Failure – no damage • Problems – overcontoured, more chances for dislodgement • Intraenamel preparation • Exception – severe abrasion or erosion.
Why we need preparation ? • Provide space • Flouride rich layer • Rough surface • Definite finish line • Location of finish line ? • Subgingivally • Area is carious or defective • Significantly dark discolouration
Instrumentation : TPS (Touati) Braeseler Kit in 1985 Advantages : Simple, coded, limited Garber (1991) Lusting (1976) Preparation Instrument
Goldstein (1984) • Lusco’s Enamel depth cutter • Labial preparation : • Uniform reduction - 0.5mm • Extreme discoloration 0.7 to 0.8 mm • 0.3mm is not recommended • 50% enamel • Begin with tracing of horizontal grooves • Cervical and middle striations – incisal / occlusal striation • Remaining areas of enamel will be removed - TFC 3 and TFC 4 – double convergence
Proximal surface : • Preservation contact area • Beyond the visible area. • TFC3 and TFC4 points • 0.8 – 1mm • Miniature rounded channel • Interlock improve the stability and mechanical properties. • Finish line : • Chamfer 0.3mm-0.5mm • Supragingival • Increased area of enamel • Moisture controle • Visual confirmation • Accessibility • Maintenance of hygiene.
Location of margins • Guided by esthetic • Contact area • Platinum foil technique – open the contact areas • Refractory cast • Why to preserve the contact area ? • Extremely difficult to reproduce. • Simplifies try-in • Saves clinical time • Simplifies bonding and finishing • Better access • Exceptions • Small proximal caries lesion • Old composite restorations • Angle fractures • Closing a diastema • Changing shape / position
Lingual surface : • Incisal edges ? • 1980s tissue conservation • Higher no. of fractures • Complete coverage of incisal edge is most preferred. • Advantages : • Angle fracture • Esthetic • Altering tooth shape • Tooth position • Occlusion to be adjusted • Easy handling and positioning • Margin to be placed outside the area occlusal impact.
Reduction – 1mm • Spherical diamond • Fine grit diamond • 20,000-60,000 rpm under air/water spray. • Prepared wet and examined dry.
PREPARATION FOR DIRECT LAMINATE VENEERS • Direct partial veneers • Outline form – extent of preparation include all defective areas. • Coarse , elliptical or round diamond • Depth of 0.5-0.75 mm • It is mandetory to extend periphery to include defect till round tooth structure. • Direct full veneers • Window preparation • Half the thickness of enamel – 0.5 to 0.75 mm midfacially, • 0.3 to 0.5mm long gingival margin.
Gingival displacement : • No special preparation of soft tissue • In case of subgingival finish line • Non medicated retraction cords • Frederick M. McInlyre (1993) • Locate CEJ • Evaluate emergence profile • Visualize the thicness • Protects gingival tissues • At the time of luting • Prevents contamination of cervical margin facilitates the finish acting as a dam. • Disinfectant surface tension reducer. Preparation sites dried. • Impressions are made
LABORATORY PROCEDURES • Choice of restorative material and technique. • Number of systems, composite technologies • Ceramic - most biomimetic - ability to simulate and to restore crown rigidity. • High thermal expansion and elasticity, unfavourable esthetics, unstable marginal integrity and decreased survival rate. • Ceramics able to compensate for structural tooth weaknesses. • Ceramic : which one ? • Cracking- feldspathic porcelian • In-Ceram spinell, procera, empress • Crack Propensity. • No Sharp angles 2) Sufficient thickness • Adequate wrapping design 3) Thorough cleaning of surface.
Choice of fabrication technique : • Ceramic fired on refractory die • Advantages : • No special equipment • Effects of colour and translucency. • Traditional feldspathic porcelain • Platinum foil technique • Data from 90s - superior marginal fidelity • Improved refractory material. • Marginal closure upto 20-40 m. • No need of ditching. Other systems are : Cast glass – ceramics (Dicor) Pressed ceramic (Empress) Slip casting (In Ceram spinell) Machined ceramics (Cerec)
Master cast in the refractory Die technique : Method : First pour – individual dies Most accurate production To verify the final fit of the restoration. Refractory dies : Control dies duplicated Two sets of replicas
Preparatory steps • Mark the margins • Dehydration firing 11000C for 5 min. • Connecting porcelain • - Sealer for the refractory surface • - Adhesive towards which the firing shrinkage should occur. • Smaller the dies better the marginal fit. • Second Pour : Solid cast • Used for final intra and interarch contact points.
Third pour : Soft tissue cast Advantages : Dies inserted interchanged Cermic layering process
Ceramic layering and finishing : 2-3 consecutive firings followed by glazing. 1) Opaque dentin firing : Situations: stained teeth and # incisal edges. light absorption at level of missing natural dentin. Dentin buildup : Higher croma in cervical region and higher value in incisal region. Cutback :
Enamel Incisal wall : • Horizontal pure enamel • Life like appearance alternating translucencies and chroma. • Buildup oversized • Dentin Characterization : • Internal effects – fluorescent and non-fluorescent stains. • High value – ideal for highlighting mamelons reduce value.
Enamel covering : • Entire facial surface • Thirds of facial surfaces covered separately. • Cervical transperant enamel. • Combination of shaded enamel – applied alternately. • Blue translucent enamel • Fired work – high value, middle third, average value cervical third and low value incisal third 60-70% of natural teeth.
Contouring : • Without alteratering essential characteristics. • Accentuation of crest and transition line angles. • Glazing and surface finishing : • Well condensed porcelain, adequate, firing - porosity. • Glazing and polishing esthetics and surface characteristics. • Diamond-silicone wheels – overglazing or autoglazing – pumice and calcium carbonate. • Attached to refractory dies. • Correction firings must be carried out only with low-fusing ceramics.
Tray-In • Cleaning the preparation • Removed the adhesive resin from spot etched area of tooth. • Sequence : • Individually placed & adaptation is checked. • Note : Excess provisional luting • All restorations - verify proximal relationship • Approval • Not to close the bite. • Acetone, ethanol, methanol, methylene chloride. • Can potentially reduce bond strength • Conditioned after try-in and not before.
BONDING PROCEDURE • Conditioning of ceramic surface • Combination of micromechanical interlocking and chemical coupling • Eg. Accu placer, Hu-friedy • A large amalgam condenser • Micromechanical interlocking • Hydrofluoric etching • Strict protective measures
Feldspathic porcelain – dissolution of glassy matrix - retentive holes and tunnels. • Ultrasonic cleaning • Reaction products of Na, K, Al, and Ca. • Ceramics with poor glossy content • Eg. In-Ceram or procera core material or pure non-crystalline ceramics eg. Ducera LFC hydrothermal glass. • Sintering of Si particles. • Lithium-base hot pressed ceramics • Lucite based hot pressed ceramics – chemical coupling
Chemical coupling : Silanization • Silica content or chemical bond • -methacryloxypropyl trimethoxy silane • Inorganic substrates and organic polymer. • Improved wettability MA MA • 4 weeks followign activation • 2-3 coats • Allowed to evaporate • Heat treatment • Dry furnace at 1000C for 5 min. • Ex. In-ceram and procera – Tribochemical silica coating
Neutral composite • Viscosity 1 Temperature Definitive insertion • Advantages : • Protects from etchent • Correct seating • Accumulation of excess Avoid air bubbles
CONDITIONING OF THE TOOTH SURFACE Enamel : 30 sec etching with 37% phosphoric acid – preparation in enamel. • Significant Dentin exposure : • Anticipated and solved tooth preparation • Dentin adhesive prior to making the impression. • Enhances bonding protection of pulp. Prevents tooth sensitivity • Final bonding, cleaned with pumice • Enamel conditioning.
Placement of ceramic restoration : • Intense light • Avoid removal of composite at interface. • Extrusion of composite at margins. • Flassing avoided crack, displacement or detach. • Chipped off by scalpel Light curing – intermittent
Opaldam • Polymerization at the marginal area - glycerin gel • Oxygen inhibition • Rapid degradation • Multiple restorations - parallel bonding procedures simulatneously on several teeth - not recommended . • If any problem in seating arises • Dipped in acetone and cleaned • Alcohol pallet – to remove resin residues. • Reconditioning of enamel • Ceramic reapplication of the silane
FINAL ADJUSTMENT AND OCLUSAL CONTROL • Immediately adjusted (maximum intercuspation) • Maintenance or re-establishment of an adequate and functional anterior guidance.
SPECIAL CONSIDERATIONS • Interdental adjustments during luting procedures • Passive fit • Care extensive wrapping and long interdental contacts • Articulating paper and abrasive
Shrinkage of luting composite • Compressive forces Vs thermal expansion • Shrinkage compressive forces • Shrinkage forces – counteract expanding forces • Water sorption • Water uptake complete relief of shrinkage stresses. • Ideal nonshrinkaging composite. Thermal expansion lowered, stress distribution within the ceramic will still be impaired. • Static stress shrinkage alone does not seem to cause crack / flaws, repeated thermal loads key role.
Prebonding cracks • Cracked procelain • Vertical eracks internal surface enlarged and adequately conditioned efficient sealing of the flare by adhesive resin will occur. • Initiating outer surface are irreparable.
Fluoridation : • Sodium fluoride (2%) is preferred to acidulated phosphate fluoride (1.23%) gels • Etching effect and damage to ceramic surface. • Chipping : • Cohesive fracture • Polished fine grain diamonds and silicon points and left as it is. • Severe cases – by sandblasting and silanization and repair it with composites.
Fracture : • Debonding at porcelain composite interface • Improper bonding • Contamination of etched surface • Improper use of silane coupling agents. • Insufficient drying • Debonding at tooth-composite interface. • Tooth substrate is dentin. • Omission of immediate dentin boding. • Postbonding cracks : • No procedure • Not a risk for the remaining underlying tooth • Can occur quite early – no progression over the years. • Replaced on patients request
Composite resin : Indirect technique restorations • Basic concept : • Cured – polymerization shrinkage • Direct technique marginal gap weakest bond strength. • Cured in laboratory – shrinkage occurs before luting composite subject to shrinkage. Less marginal gap. • Advantages : • Accelerated wear of opposing natural tooth • Composites can be adjusted and repolished easily. • Can be repaired
Composite resin systems : • Microfilled resins • Small particle composite resins • Hybrid resins • Acid etched or silanated • New category of processed composite has introduced. • Polymer-glass, polymer-cermaic, ceromer (ceramic-optimized polymer)
Apply layers of dentin, enamel, and incisal shades and cure each layer for 40 seconds • Remove the veneers from the flexible model. • Contour and polish the veneers 12 and 30 fluted finishing carbide burs in a high-speed hand piece or porcelain contouring and polishing wheels on a lathe. • Place the veneers on the original stone model to check the fit and margins. • Curing as per the manufacturers instruction • These praessed composites canbe conditioned and bonded in a similar manner as the porcelain laminates.