Download
1 / 77
830 likes | 1.43k Views
Otitis & Pharyngitis in Peds Chp 121 Tintinalli. 4/13/06 Dr. Batizy Slides by Bogdan Irimies. Otitis Media: definitions. Otitis media: inflammation of middle ear Acute otitis media (AOM): s/sx’s of infection, otalgia, otorrhea, fever, irritability, anorexia or vomiting.

E N D
Otitis & Pharyngitis in PedsChp 121 Tintinalli 4/13/06 Dr. Batizy Slides by Bogdan Irimies
Otitis Media: definitions • Otitis media: inflammation of middle ear • Acute otitis media (AOM): s/sx’s of infection, otalgia, otorrhea, fever, irritability, anorexia or vomiting. • Otitis media w/effusion(OME): asymptomatic collection of fluid in middle ear
Otitis Media: • OME: duration can be divided into: • Acute <3 wks • Subacute 3wks-3 mos • Chronic >3 mos. Most important distinction between OME and AOM is the s/sx’s of acute infection (otalgia, otorrhea,fever) are lacking in OME.
Acute Otitis Media: • Peak incidence b/w 6-18 mos. • Bacteria most common organism, isolated 60-75% of cultures • Bacteria colonize the nasopharynx and enter middle ear thru Eustachian Tube.
Acute Otitis Media: Organisms • Strep. Pneumoniae 40-50% • H. Flu 30-40% • M. catarrhalis 10-15% • GABHS/Strep. Pyogenes & Staph. Aureus 2% • Chlamydia pneumonia in those <6 mos old
Acute Otitis Media: Pathophysiology • Abnormal function of eustachian tube appears to be dominant factor: obstruction and abnormal patency • Upper respiratory tract infections or allergies can cause obstruction and decrease ET function • Abnormal Patency may allow reflux of nasopharyngeal secretions
Acute Otitis Media: Clinical Features • Otalgia, otorrhea, fever, ear pulling & irritability (especially in infants) • Most important diagnostic tool is pneumatic otoscopy • Light reflex is no diagnostic value • TM of AOM: • Opaque, pale yellow, red, bulging and bony landmarks are lost, loss of or decrease in mobility of TM
Acute Otitis Media: Treatment • Selection of ATBX is based on the following factors: • 1. Knowledge of likely etiologic agent or recovery of specific pathogen from middle ear • 2. Efficacy of specific ATBX’s for responsible organisms • 3. ATBX penetration into middle ear fluid • 4. Drug allergy hx • 5. Compliance • 6. Drug side effects • 7. Treatment failure or success of previous drug regimens for that child
Acute Otitis Media: Treatment • High dose Amoxicillin is 1st line • Due to prevalence of Drug resistant strep. Pneumoniae(DRSP) • Dose is 80-90 mg/kg/day • High risk patients for DRSP: • ATBX w/in past 3 mos • Day Care • Age < 2 y/o
Amox-Clav TMP/SMX Cefaclor/cefuroxime/Cefprozil/Cephalexin Cefdinir/ceftriaxone Azithromax/Clarithromycin 10 day course for all ATBX (except Zithro) If after 3 days of treatment and still AOM: High dose amox-clav Cefuroxime IM Ceftriaxone (50 mg/kg /day) for 3 consecutive days Cefdinir(Omnicef) Acute Otitis Media: Other Options
Acute Otitis Media: Special Treatment • PCN Allergy: Clinda, Erythromycin, TMP/SMX, clarithromycin, azithromycin • Infant < 2wks old: • GBS, S. aureus, Gram neg. Bacilli • Full septic W/U: CBC, Blood cx’s, UA/C&S, LP/CSF C&S, CXR • Admit for IV ATBX: amp + Gent or ceftriaxone • If 2-6 wks old: possible septic W/U depending on appearance of infant, available close follow up
Acute Otitis Media: Additional Therapy • Antipyretics • Analgesics: Auralgan instilled into EAC (don’t use if TM perforated) • Peds should F/U 10-14 days after completion of ATBX therapy
Recurrent Otitis Media: • Definition: 3 or > of AOM in 6 mos or 4 episodes of AOM w/in 12 mos with at least 1 episode w/in past 6 mos. • Risk factors: onset of AOM < 1 y/o, day care, genetic susceptibility/family hx • Tx: prophylactic ATBX • Amox 20mg/kg/d for 3-6 mos • If fail ATBX, myringotomy w/tympanostomy tube insertion
Persistent Otitis Media: • Defined as presence of AOM w/in 3 days of Tx or recurrence of s/sx’s w/in completion of 10 day ATBX course • Caused by either relapse or reinfection • Tx: High dose amox-clav/cefdinir/ cefuroxime/IM ceftriaxone x 3 days
Chronic Suppurative Otitis Media: CSOM • Defined as persistence > 6 wks of a chronic inflammation of middle ear and mastoid in the presence of perforated or non-intact TM. • Usually the sequela of partly treated or untreated AOM or recurrent AOM • Ofloxacin otic for peds >12 y/o and for AOM in peds > 1 y/o w/T-tubes or non-intact TM’s.
Hearing loss TM perforation or retraction Tympanosclerosis Adhesive OM Ossicular discontinuity CSOM Cholesteatoma Mastoiditis Petrositis Labyrinthitis Facial paralysis Complications & Sequelae of OM:
Complications & Sequelae of OM: • Intracranial complications: • meningitis • extradural abscess • subdural empyema • focal encephalitis • Brain abscess • Sigmoid sinus thrombosis • Otic hydrocephalus
Otitis Media w/Effusion: OME • Collection of fluid in middle ear w/out acute s/sx’s of infection. Usually follows an episode of AOM. • Hearling loss is most prevalent and dangerous complication of OME • Cognitive linguistic and speech development is affected
Otitis Media w/Effusion: OME • Management options: • Peds 1-3 y/o w/OME for at least 3 mos: obs w/no treatment or treatment w/ATBX for 10-14 days • Peds w/ OME for at least 3 mos and hearing loss: refer to ENT for T-tubes • T-Tubes remain in for few wks to several years
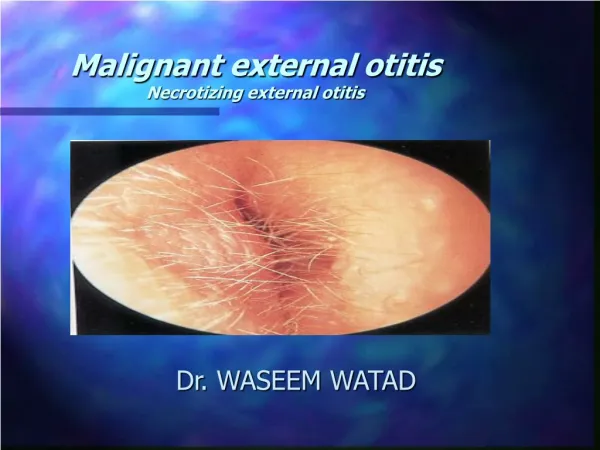
Otitis Externa: • Def: inflammatory condition of auricle, external ear canal or outer surface of TM. • Caused by infection, inflammatory dermatoses, trauma or any combination of the 3. • Pathogenic organisms: P. aeruginosa, S. aureus, fungi
Otitis Externa: • Clinical s/sx’s: itching, sense of fullness in ear, pain, redness, edema, tenderness of canal, cheesy/purulent drainage from canal. • Otomycosis: OE caused by fungus, Aspergillus niger, intense itching, more common w/underlying immune disorders and Diabetes mellitus
Otitis Externa: Treatment • Atraumatic cleaning of the ear is most important step, can use gentle suctioning • Mild OE: cleaning & acetic acid eardrops (Otic Domeboro) 3-4 x a day for 1 week. • Moderate OE: cleaning plus ATBX drops such as neomycin & polymyxin B, Floxin Otic, Cipro HC • Otomycosis: 2% acetic acid
Pharyngitis: Non-Streptococcal • Most are caused by viruses: adenovirus, EBV, influenza virus, parainfluenza, rhinovirus, herpes simplex, enterovirus. • Clinically difficult to distinguish from Group A Beta hemolytic Strep.(GABHS). • Other non-GABHS causes are Corynebacterium diphtheriae, N. gonorrhea, HIV 1.
Pharyngitis: Non-Streptococcal • C. diptheria: cause of pharyngitis in developed countries • Infectious invasion can produce tissue necrosis and pseudomembrane that can cause airway obstruction. • Produces an exotoxin that can cause wide spread organ damage: myocarditis, cardiac dysrhythmia, neuritis w/bulbar and peripheral paralysis, nephritis, and hepatitis • TX: PCN or erythromycin and horse serum anti-toxin
Pharyngitis: Non-Streptococcal • N. gonorrhea: cause of pharyngitis in sexually active adolescents • Maybe asymptomatic or cause mild symptoms w/exudative tonsillitis and/or cervical lymphadenopathy • Obtain rectal/vaginal/urethral cx’s and test for Hep. B and syphilis when suspected • Tx: ceftriaxone 125 mg IM x 1
Pharyngitis: Non-Streptococcal • EBV: • Herpes virus that causes Infectious mononucleosis(IM) • Classic IM: malaise, fatigue, fever, sore throat, adenopathy, organomegally • Can be co-infected w/EBV & GABHS • Supportive treatment (fluids,rest, acetaminophen)
Pharyngitis: Non-Streptococcal • HIV: can produce an IM like syndrome w/fever, sore throat, adenopathy • Can have GI and mucocutaneous symptoms which occur more likely w/HIV v/s IM infection
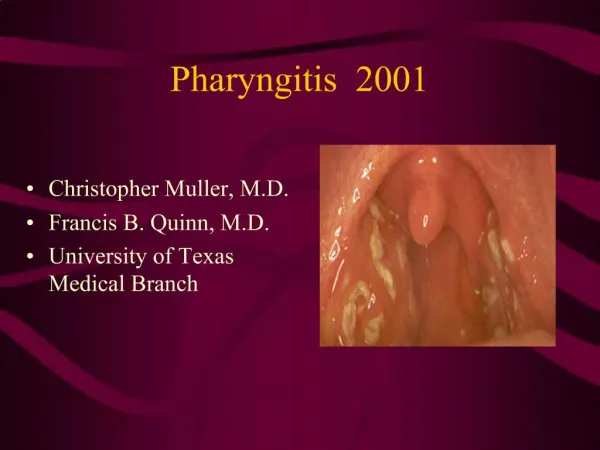
Streptococcal Pharyngitis: • Peak months are Jan.-May • Peak ages 4-11, GABHS uncommon < 3 y/o • Characteristic s/sx’s • Fever, sore throat, erythema of tonsils & pharynx, exudate of tonsils & pharynx, erythema & edema of uvula, petechiae of soft palate, enlarged tender ant. Cervical lymph nodes, scarlatiniform rash
Streptococcal Pharyngitis: • Headache, vomiting, abd. Pain, meningismus and torticollis can also occur • Coughing, rhinorrhea or ulceration suggest alternative diagnosis
Streptococcal Pharyngitis: • Dx: • Multitude of rapid antigen procedure including ELISA, latex agglutination, coagglutination • Sensitivity 85-90%, specificity 98-100% under ideal conditions but more like sensitivity of 50% • False positive rate is low, false neg. rate is high • If test is +, treat GABHS, if neg, send throat culture
Streptococcal Pharyngitis: Tx • Objectives to treat GABHS are: • Prevent rheumatic fever • Prevent suppurative complications (peritonsillar/retropharyngeal abscess, cellulitis, suppurative cervical lymphadentis • Hasten clinical recovery
Streptococcal Pharyngitis: Tx • PCN G IM 600,000 units if <27 kg or 1.2 million units IM if > 27 kg (good choice if compliance an issue) • Oral PCN 250-500 mg bid x 10 days • Amoxicillin soln for peds unable to swallow pills • PCN allergy: erythromycin or cephalosporin
Streptococcal Pharyngitis: Tx • Recommended peds w/GABHS infection receive ATBX for 24 hrs before returning to school/day care • Summary: if rapid test is +, treat. • If classic clinical finding or a scarletiniform rash is present, treat regardless of rapid test.
Streptococcal Pharyngitis: Complications • Overall incidence of rheumatic fever <1:100,000 in U.S. • Post-strep. Glomerulonephritis is not prevented w/ATBX, related to nephritogenic strain of streptococci • Invasive GABHS infections include: • Septicemia, toxic shock like syndrome, pneumonia, cellulitis, lymphangitis, necrotizing fasciitis
Skin and Soft Tissue Infections Chp 122 Tintanalli Dr. Batizy Slides by Bogdan
Conjunctivitis: • Inflammation of the conjunctivae • Result of infection, allergy, mechanical or chemical irritation • In newborns: Chlamydia trachomatis & N. gonorrhea • Children: adenovirus, Hemophilus species, strep. pneumoniae
Photophobia Ocular pain or pruritus Foreign body sensation Conjunctival erythema Crusting of the eyelids Conjunctivitis: Clinical
Conjunctivitis: Clinical • Examination for: visual acuity, visual fields, EOM function, periorbital area, eyelid eversion, conjunctiva fluorescein staining of cornea, pupillary reflex, anterior chamber, and fundus. • In conjunctivitis: erythema, increased secretions, cornea stain is neg. except if herpetic keratitis and adenovirus, visual acuity is normal • Gram stain only is neonates or confusing cases
Infectious Conjunctivitis Orbital/periorbital cellulitis Foreign body Corneal abrasion Uveitis Glaucoma Allergic conjunctivitis Chronic Seasonal Pruritus Symptoms of allergic rhinitis D/Dx: Red Eye