Download
1 / 3
50 likes | 329 Views
Drug Resistance. Mono-resistant TB – resistant to only one drug Poly-resistant TB – resistant to more than one drug but not the combination of isoniazid and rifampicin. Multidrug-resistant TB (MDR-TB ) TB caused by bacteria resistant to at least isoniazid and rifampicin.

E N D
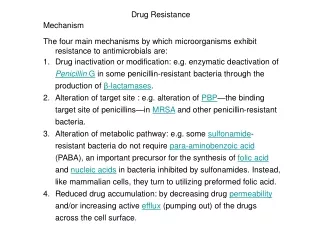
Drug Resistance Mono-resistant TB – resistant to only one drug Poly-resistant TB– resistant to more than one drug but not the combination of isoniazid and rifampicin. Multidrug-resistant TB (MDR-TB) • TB caused by bacteria resistant to at least isoniazid and rifampicin. Extensively drug-resistant TB (XDR-TB) • TB caused by bacteria resistant to isoniazid and rifampicin (i.e. MDR-TB) plus any fluoroquinolone and any second-line anti-TB injectable drugs (amikacin, kanamycin or capreomycin) There is an estimated 150 000 deaths per year from MDR-TB alone.
Result from either primary infection with resistant bacteria or may develop secondarily in the course of treatment due to inadequate treatment regimens or poor compliance. • Risk factors include – • Previous treatment for TB especially if prolonged • Contact with a patient known to have drug resistant TB or live in an area with high drug-resistant TB prevalence • Immunocompromised (HIV in particular) • Poor compliance • Culture +ve after 2 months treatment • Can take up to 2 years to treat with drugs less potent, more toxic and more expensive. Higher mortality rate.
Treatment is based on sensitivity testing with at least 3 drugs and an initial bactericidal injectable agent. • Fluoroquinolone should be used where possible. • XDR-TB Linezolid becomes mainstay treatment. Surgery is a limited option if disease localised.