Download
1 / 66
670 likes | 842 Views
EKG 101. Deborah Goldstein Georgetown University Department of Internal Medicine. Steps to Interpreting an EKG. Rate Rhythm Axis Intervals (PR, QRS, QTc) Hypertrophy ST segments T waves Q waves. Rate. Naming stuff. Normal Sinus Rhythm. P before every QRS

E N D
EKG 101 Deborah Goldstein Georgetown University Department of Internal Medicine
Steps to Interpreting an EKG • Rate • Rhythm • Axis • Intervals (PR, QRS, QTc) • Hypertrophy • ST segments • T waves • Q waves
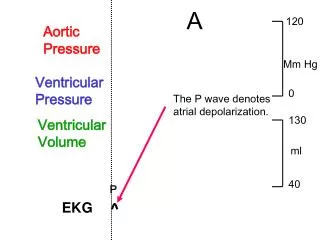
Normal Sinus Rhythm • P before every QRS • Best places to look: II, V1 • QRS after each P
Axis 1. The direction of the mean electrical vector, representing the average of current flow in the frontal plane. 2. Normal axis: –30 to +90 degrees.
Axis • Look at lead I and aVF. • Then find the isoelectric lead (where the QRS complex is most nearly biphasic). • Then go 90 degrees perpendicular to the isoelectric lead.
Ddx of Axis Deviation LAD • Left ventricular hypertrophy, Left anterior fascicular block, LBBB, Inferior wall MI • Pregnant, ascites, short/fat RAD • Right ventricular hypertrophy, Left posterior fascicular block, RBBB, lateral wall MI • PE
PR Interval • Normal PR = 0.12 – 0.20 seconds (3-5 little boxes) • Long PR >0.20 seconds (>5 little boxes) =Delayed conduction from atria to ventricles • First-degree AV block • PR>0.20 seconds • NO dropped QRS
Second Degree AV Block • Wenckebach (Type 1) =block within AV node • PR interval progressively lengthens...then dropped QRS • Mobitz (Type 2) =block within His-Purkinje system • Fixed PR with dropped QRS • WORSE! • Sarcoid, Lyme.... • Pacemaker!
Third Degree AV Block =Failure of conduction of any atrial impulses to get to the ventricles =Complete AV block Causes of Acute AV Block: • Calcium channel blockers • Acute RCA occlusion • Digoxin toxicity
QRS Interval Normal = 0.06-0.10 seconds Wide QRS = >0.12 seconds (>3 little boxes) • PVC...if >3 in a row or >6/min=VTach • RBBB, LBBB • Left fascicular hemiblock • Hyperkalemia Narrow QRS= <0.06 sec • SVT (150-250 bpm) • Idiojunctional rhythm (40-60 bpm) • Premature junctional complex
Chest Leads V6 V1
Bundle Branch Block V1-V2 = Right precordial leads V5-V6 = Left precordial leads LBBB • Rabbit ears in V6 represent delay between depolarization from the septum to the LV RBBB • Rabbit ears in V1 represent delay between depolarization from the septum to the RV
V1 V6 Normal: V1: rS complex V6: qR complex RBBB: V1: Rabbit Ears (rSR) V6: qRS complex LBBB: V1: wide QS complex V6: Rabbit Ears
QT Interval • Should be < ½ (R-R’ interval) • Measure from the start of the QRS to end of T wave • Varies with heart rate, so correct for RR interval • Normal QTc: women=0.44, men=0.42 • QTc = QT (#of small squares) x 0.04 √RR • Long QT can lead to ‘R on T’Death
Causes of Long QT **Think ‘Lytes and Meds first! • Low K, Low Ca, Low Mg • Macrolides, Quinolones • All Antipsychotics (Haldol worst, Geodon least) • SSRIs • Sotalol, Quinidine, Ondansetron, Amio, TCAs • Pts w/LVH or CHF are predisposed to medication-related lengthening of QT interval! • Avoid Macrolides, Quinolones in them!
Long QT: Less common causes • Hypothyroid • Hypothermia • AV Block • MI • CVA • Head injury • Congenital long QT
Atrial Enlargement RAE • P wave is tall and peaked (>2.5mm high) • OR Biphasic P wave with initial positive inflection • Ddx: Pulmonary HTN, COPD, PE LAE • P wave is wide (>0.12 sec) and notched in the middle “M” • OR Biphasic P wave with terminal negative inflection • Ddx: Systemic HTN, Aortic Insufficiency, Mitral Stenosis
Which Atria is Enlarged? II V1
LVH Criteria • Sokolow + Lyon • S V1+ R V5 or V6 > 35 mm • Cornell criteria (Circulation, 1987;3: 565-72) • S V3 + R avl > 28 mm in men • S V3 + R avl > 20 mm in women • Framingham criteria (Circulation,1990; 81:815-820) • R avl > 11mm, R V4-6 > 25mm • S V1-3 > 25 mm, S V1 or V2 + • R V5 or V6 > 35 mm, R I + S III > 25 mm • Romhilt + Estes (Am Heart J, 1986:75:752-58) • Point score system (Am Heart J, 1999;37:161)
ST changes: axis + anatomy • Lateral: • I, aVL • LCA, CFX • Anterior: • V1, V2, V3, V4 • LAD Inferior: -II, III and aVF -RCA (or LCA) Memorize this slide
Q waves • Normal Q wave: • Small septal Qs in I, aVL, V5, V6 • Isolated Qs in III, V1 • Pathologic Q wave: • wider than 1 small box (0.04 sec) • OR >25% height of the R wave in that complex
Non-ST Elevation MI =Severe subendocardial ischemia • Marked, diffuse ST depressions in I, II, III, aVL , aVF , V2-V6
Acute ST Elevation MI • Normal • Hyperacute • T wave Elevation • Acute • ST Elevation • Hours Later • ST Elev, Q begins to form, T wave inverts • Days Later • Q wave, T wave inversion • Weeks Later • Q wave
Acute Inferior Wall MI • ST elev in II, III, AVF • Reciprocal ST depression in anterior leads (V2-V4) =RCA occlusion (some LCx)