Download
1 / 19
190 likes | 297 Views
False Positive ST Elevation in Patients Undergoing Direct Percutaneous Coronary Intervention. David M. Larson MD, Katie M. Menssen, BS,, Scott W Sharkey MD, James Harris MD, Jeffrey T. Meland, MD Robert Schwartz MD, Barbara T Unger RN, Timothy D. Henry MD,

E N D
False Positive ST Elevation in Patients Undergoing Direct Percutaneous Coronary Intervention David M. Larson MD, Katie M. Menssen, BS,, Scott W Sharkey MD, James Harris MD, Jeffrey T. Meland, MD Robert Schwartz MD, Barbara T Unger RN, Timothy D. Henry MD, Ridgeview Medical Center, Waconia, Minnesota and Minneapolis Heart Institute Foundation, Minneapolis, Minnesota
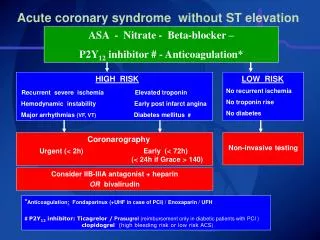
Introduction • Previous data shows that up to 11% of STEMI patients treated with thrombolysis did not have a Myocardial Infarction (MI) • ACC/AHA guidelines recommend that the Emergency physician make the decision regarding reperfusion therapy for STEMI • There is limited data reporting the rate of “false positive” ECGs in STEMI patients treated with Percutaneous Coronary Intervention.
Objective • To determine the incidence and etiologies of “false positive” ECGs, defined as: no culprit coronary vessel and negative cardiac markers (no MI), from a non-selected cohort of STEMI patients. • To determine the incidence of “true false positive” ECGs defined as no culprit, no significant coronary disease and negative cardiac markers.
Methods • Minneapolis Heart Institute/Abbott Northwestern Hospital (ANW) – a tertiary cardiac center with referral relationships with 30 community hospitals (CH) in Minnesota and Wisconsin – instituted the “MHI Level 1 MI Program” in 2003.
Methods • Level 1 MI Protocol: Includes STEMI (ST elevation or new Left Bundle Branch Block) with symptom < 24hrs. Diagnosis and decision to activate the cath lab is made by the Emergency Physician at the presenting hospital. Transferred patients go directly to cath lab for Primary or Facilitated PCI • Data obtained from a prospective registry of all “Level 1 MI” patients that includes clinical, laboratory, ECG, angiographic and follow up data.
What is the prevalence and etiology of “False Positive” Cath Lab Activation? STEMI Larson, DM et al JAMA 2007;298(23):2754-2760
The Clinical Challenge Denying Reperfusion Falsely Declaring an Emergency Larson, DM et al JAMA 2007;298(23):2754-2760
Definitions of “False Positive” Cardiac Cath Lab Activation • No culprit • No significant coronary disease • Negative cardiac biomarkers Larson, DM et al JAMA 2007;298(23):2754-2760
Results from the Level 1 MI Program • From 3/03 to 11/06, 1,345 STEMI patients enrolled in Level 1 MI program including 1,048 transferred from 30 rural or community hospitals. • 149 (11.2%) had normal cardiac biomarker levels. Larson, DM et al JAMA 2007;298(23):2754-2760
“False Positive” Cath lab Activations STEMI Diagnosis N=1,345 5 died prior to angio 5 Case canceled Angiography N=1,335 Larson, DM et al JAMA 2007 Multiple potential culprits N=10 (0.7%) No Angiographic Culprit N=187 (14%) Clear culprit N=1138 (85.3%
No Culprit N=187 (14%) Mod-Severe CAD N =60 (4.5%) No Significant CAD N = 127 (9.5%) Positive Cardiac Markers N= 16 (27%) Negative Cardiac Markers N = 44 (73%) Positive Cardiac Markers N= 48 (38%) Negative Cardiac Markers N = 79 (62%)
With a culprit Clear culprit N=1138 Multiple Potential Culprits N=10 Positive Cardiac Markers N= 1112 Negative Cardiac Markers N = 26 Positive Cardiac Markers N= 10 Negative Cardiac Markers N = 0 Larson, DM et al JAMA 2007
No Angiographic Culprit N=187 (14%) Negative Cardiac Markers N = 123 (9.2%) Positive Cardiac Markers N= 64 (4.8%) Larson, DM et al JAMA 2007
No culprit and negative markers by Hospital ED Volume ED visits/year Not significant Larson, DM et al JAMA 2007
Left Bundle Branch Block • New or presumed new LBBB observed in 36 (2.6%) of patients • No culprit: 16 (44%) • No significant CAD: 10 (27%) • Negative cardiac biomarkers: 13 (36%) • 30 day mortality in those with new LBBB was 8.3% Larson, DM et al JAMA 2007;298(23):2754-2760
Gender differences • 381 (28.3%) women enrolled in Level 1 registry • No culprit: 17.1% women vs 12.7% men (p=0.04) • No significant CAD: 13.6% women vs 7.9% men (p=0.001) • Negative biomarkers: 12.3% women vs 10.6% men (p=0.36) • Stress cardiomyopathy may account for differences Larson, DM et al JAMA 2007;298(23):2754-2760
Summary: Incidence of “False Positive” Cath Lab Activation • No culprit: 14% • Normal or Minimal CAD: 9.5% • Negative cardiac markers: 11.2% • Combination of no culprit and negative biomarkers: 9.2% Larson, DM et al JAMA 2007;298(23):2754-2760
Conclusions • The incidence of “false positive” ECGs in STEMI patients treated with Primary PCI is similar to previous data in patients treated with thrombolytic therapy. • Patients presenting with “False Positive” ST elevation are a heterogeneous group, many with other serious cardiac conditions.