Download
1 / 77
870 likes | 1.21k Views
polycystic ovary syndrome in adolescents. DR. Nedaa Bahkali 2012. Menstrual cycles are often irregular in the first months after menarche. According to a study by WHO : the median length of the first cycle after menarche was 34 days,

E N D
polycystic ovary syndrome in adolescents DR. NedaaBahkali 2012
Menstrual cycles are often irregular in the first months after menarche. • According to a study by WHO : • the median length of the first cycle after menarche was 34 days, • with 38%of the cycles > 40 days and 7 % occurring <20 days apart . World Health Organization multicenter study on menstrual and ovulatory patterns in adolescent girls, J Adolesc Health Care. 1986
Menstrual disorders and abnormal uterine bleeding (AUB) are among the most frequent gynecologic complaints of adolescents account for 50% . • Menstrual disorders in adolescence: pathophysiology and treatment, Horm Res., 1991,Belgique. • Menstrual disorders during adolescence, PediatrEndocrinol Rev. 2006, University of Athens, Greece.
Polycystic ovary syndrome (PCOS) accounts for the vast majority of anovulatory symptoms and hyperandrogenism in adolescent . • PCOS is the most common endocrine abnormality of reproductive-aged women in the United States. • The prevalence and features of the polycystic ovary syndrome in an unselected population, The University of Alabama at Birmingham, J Clin Endocrinol Metab. 2004. • The diagnosis of PCOS has life-long implications with increased risk for infertility, metabolic syndrome, type 2 diabetes mellitus, and probably cardiovascular disease.
The classic syndrome originally was described by Stein and Leventhal as the association of amenorrhea with polycystic ovaries, and variably, hirsutism and obesity. • J ObstetGynecol 1935
It is now recognized that PCOS represents a spectrum of disease characterized primarily by the following features:
controversy arises from the fact that a polycystic ovary is often a normal variant and some asymptomatic ovulatory girls have subclinical PCOS according to the Rotterdam-AES criteria .
None of these criteria fully addresses some of the unique problems in diagnosing PCOS in adolescents. As an example, even in girls without PCOS, approximately one-half of menstrual cycles are anovulatory in the first two years after menarche . • Hyperandrogenism during puberty and adolescence, and its relationship to reproductive function in the adult female. In: Reproductive Medicine, Raven Press, 1993. • Furthermore, polycystic ovaries may be missed by the Transabdominal ultrasound technique that is typically used for virginal adolescents, particularly if they are obese.
Evaluation for PCOS is recommended in the following clinical scenarios: • Girls with a sole finding of moderate or severe hirsutism, or a hirsutism equivalent, including persistent acne , or pattern alopecia • Girls with mild hirsutism or obesity with any other feature of PCOS (eg, menstrual abnormality) • Adolescent girls with menstrual irregularity that persists more than two years or who have severe dysfunctional uterine bleeding • Adolescent girls with intractable obesity whether or not hirsutism, hirsutism equivalents, or menstrual irregularity are present
Evidence of ovarian dysfunction • Menstrual irregularity constitutes evidence of ovarian dysfunction. • However, normal menstrual regularity does not mean ovulatory function is normal. • A polycystic ovary is considered evidence of ovarian dysfunction in the setting of hyperandrogenism when menses are regular.
TESTING FOR ANDROGEN EXCESS • The key androgen to measure is serum (or plasma) testosterone. • Serum total and free testosterone: • best assessed in the early morning. • on days 4 through 10 of the menstrual cycle in regularly cycling women; norms are standardized for this part of the menstrual cycle. • Oral contraceptive pills interfere with the assessment of androgens. • They suppress gonadotropins, elevate sex hormone binding globulin (SHBG), and directly inhibit steroidogenic enzymes such as 3ß-hydroxysteroid dehydrogenase. • After discontinuing oral contraceptive pills, normal women may transiently have a slightly high total testosterone level but a normal free testosterone level because SHBG turnover is slower than testosterone turnover. • Clinical practice. Hirsutism, N Engl J Med. 2005, Department of Pediatrics and Medicine, University of Chicago, USA.
Total testosterone : • The normal upper limit for serum total testosterone in women is approximately 60 ng/dl (2.0 nmol/L) . • Free testosterone : • An elevation in serum (or plasma) free testosterone is the single most sensitive test to establish the presence of hyperandrogenemia. • The serum free testosterone concentration is about 50 percent more sensitive for the detection of hyperandrogenemia than the total testosterone concentration. • This is because elevated insulin levels (a frequent concomitant of PCOS) and elevated androgen levels both act to inhibit hepatic production of sex hormone-binding globulin (SHBG), which is the main determinant of the bioactive portion of serum testosterone, the fraction that is free or "bioavailable" the latter including the fraction that is loosely bound to albumin.
If hyperandrogenemia is revealed by the laboratory testing, the patient should be further evaluated to identify the underlying cause of androgen excess. The diagnosis of PCOS is made when other hyperandrogenicdisordersexcluded,,
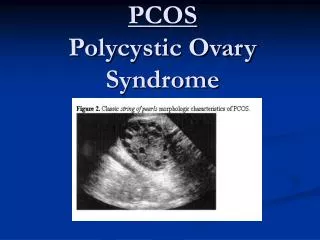
Ultrasonography • International consensus criteria define a polycystic ovary on the basis of either excessive size or follicle number (or both), in the absence of a dominant-size follicle (>1.0 cc) or a corpus luteum. • Using these criteria, a polycystic ovary can be identified by ultrasonography in about 75 % of women with PCOS.
Ultrasonography • Excessive ovarian size is defined as • an ovary with a volume >10.5 mL in adults • >10.8 mL in adolescents. • An alternate measure of increased volume is a maximal area >5.5 cm2. Most polycystic ovaries in PCOS are enlarged. • Excessive follicle number is defined • by vaginal ultrasonography as a total follicle count of ≥12 per ovary. • In adolescents in whom abdominal rather than vaginal ultrasonography is indicated, it is defined as ≥10 follicles per maximum plane . • These follicles are typically 2 to 9 mm in diameter. • Asymptomatic volunteers with a polycystic ovary are a functionally distinct but heterogeneous population, J Clin Endocrinol Metab. 2009, Section of Adult and Pediatric Endocrinology, The University of Chicago , USA.
Ultrasonography • The transabdominalultrasonographic approach that is standard and appropriate in virginal adolescents may underestimate the prevalence of polycystic ovaries in comparison with the transvaginal approach used in adult women . • This difference is modest. • In a prospective study of patients with PCOS in which these criteria were used , a polycystic ovary was found in 69 percent of adolescents and 87 percent of adults (p = 0.12, unpublished data). • The advantage of the transabdominal approach is that a screening for an adrenal mass is facilitated. • Asymptomatic volunteers with a polycystic ovary are a functionally distinct but heterogeneous population, J Clin Endocrinol Metab. 2009, Section of Adult and Pediatric Endocrinology, The University of Chicago , USA. • Gynecologic imaging: comparison of transabdominal and transvaginalsonography, Radiology. 1988, Department of Radiology, West Penn Hospital, Pittsburgh, PA
Ultrasonography • While a polycystic ovary is a criterion for ovarian dysfunction in the setting of hyperandrogenism, in the absence of hyperandrogenism a polycystic ovary is usually a normal variant. • Polycystic ovaries are common in the general population,found in about 10 % of regularly menstruating adolescents. • Polycystic ovaries in adolescents and the relationship with menstrual cycle patterns, luteinizing hormone, androgens, and insulin, FertilSteril. 2000, Division of Reproductive Endocrinology and Fertility, VrijeUniversiteit Medical Center, Amsterdam, The Netherlands.
ADDITIONAL EVALUATION OF PCOS PATIENTS • Once a diagnosis of PCOS has been established, identifying abnormal glucose tolerance or other features of the metabolic syndrome is important because PCOS is a risk factor for the early development of type 2 diabetes mellitus, metabolic syndrome, and their associated risks for sleep-disordered breathing and cardiovascular risk sequelae . • Polycystic ovary syndrome is associated with obstructive sleep apnea and daytime sleepiness: role of insulin resistance, J Clin Endocrinol Metab. 2001, Sleep Research and Treatment Center, Department of Psychiatry, Penn State University College of Medicine, USA. • Relationships between sleep disordered breathing and glucose metabolism in polycystic ovary syndrome, J Clin Endocrinol Metab. 2006, Department of Medicine, University of Chicago, Chicago, USA.
About a quarter of adolescents with PCOS meet proposed adolescent criteria for the metabolic syndrome [17,23,24].
screening for abnormal glucose tolerance, performing an oral glucose tolerance test (OGTT) in adolescents with obesity or other risk factors for diabetes mellitus, even if the fasting blood sugar is normal. • This is the recommendations made by the Rotterdam workshop ,the American Association of Clinical Endocrinologists, and the Androgen Excess and PCOS Society in adult women with PCOS.
The prevalence of diabetes was reported to be 2 % based on the fasting blood sugar in one series, • and 8 % when based on OGTT criteria in another series of adolescents. • In both series, almost all of the adolescents had no symptoms of diabetes. • Relationship of adolescent polycystic ovary syndrome to parental metabolic syndrome, J Clin Endocrinol Metab. 2006, University of Chicago Comer Children's Hospital, Section of Pediatric Endocrinology, USA. • Adolescent girls with polycystic ovary syndrome have an increased risk of the metabolic syndrome associated with increasing androgen levels independent of obesity and insulin resistance, J Clin Endocrinol Metab. 2006, Division of Endocrinology, Metabolism, and Molecular Medicine, Northwestern University Feinberg School of Medicine, Chicago, USA
In patients with PCOS: • Glucose tolerance should be monitored regularly because a substantial number will experience deterioration in glucose tolerance. • As an example, among 25 adolescent and young women followed for a mean of 34 months, the two hour blood glucose deteriorated at an average of 9 mg/dL (0.5 mmol/L) per year . • Among the 14 women with PCOS and normal glucose tolerance at baseline, 55 percent experienced deterioration of glucose tolerance when they were retested with an OGTT. • Among the 14 women with PCOS and impaired glucose tolerance at baseline, 29 percent progressed to diabetes. • Prevalence of impaired glucose tolerance and diabetes in women with polycystic ovary syndrome, Diabetes Care. 1999, Department of Medicine, University of Chicago, Illinois, USA.
PCOS is a risk factor for endometrial carcinoma. • The basis of the risk is multifactorial: • arise from the combined effects of unopposed estrogens on the endometrium, caused by chronic oligo-anovulation • and progesterone resistance, obesity, hyperinsulinemia, and hyperandrogenism. • Polycystic ovary syndrome and endometrial cancer, SeminReprod Med. 2008, University Department of Obstetrics and Gynaecology, Royal Free and University College Medical School, University College London, London, United Kingdom. • Polycystic ovary syndrome increases the risk of endometrial cancer in women aged less than 50 years: an Australian case-control study, Cancer Causes Control. 2010, School of Population Health, The University of Queensland, Herston Road, Herston, QLD 4006, Australia. • Progesterone Resistance in PCOS Endometrium: A Microarray Analysis in Clomiphene Citrate-Treated and Artificial Menstrual Cycles, J Clin Endocrinol Metab. 2011, Department of Obstetrics and Gynecology, Greenville Hospital System, Greenville, South Carolina .
There is a high frequency of PCOS and metabolic syndrome among immediate relatives of individuals with PCOS. • According to one study, • approximately one-half of sisters of PCOS have an elevated serum testosterone level, • and half of these in turn have menstrual irregularity and thus meet NIH criteria for PCOS . • Evidence for a genetic basis for hyperandrogenemia in polycystic ovary syndrome, Proc Natl Acad Sci U S A. 1998 Department of Obstetrics and Gynecology, Pennsylvania State University College of Medicine, Hershey, PA 17033, USA.
In another study, • ¼ of sisters met Rotterdam criteria for PCOS, having hyperandrogenism and a polycystic ovary, although menses were ovulatory . • Ovarian morphology is a marker of heritable biochemical traits in sisters with polycystic ovaries, J Clin Endocrinol Metab. 2008, Institute of Reproductive and Developmental Biology, Imperial College London,UK.
Treatment for PCOS in adolescents is directed at the following clinical manifestations: • Menstrual irregularity • Cutaneous hyperandrogenism, primarily hirsutism and acne . • Obesity and insulin resistance.
Menstrual irregularity should be treated in adolescents with PCOS: • chronic anovulation increases the risk of developing endometrial hyperplasia, which is associated with endometrial carcinoma. • Anemia can result from dysfunctional uterine bleeding or menorrhagia.
Combination OCPs • the first-line treatment. • OCPs induce regular menstrual periods with a higher degree of reliability than other forms of treatment.
Combination OCPs • Norgestimate: • a potent progestin with low androgenic effect and is combined with ethinyl estradiol: 35 mcg (in Ortho-Tri-Cyclen®). • It is especially useful for patients with associated acne vulgaris, for which it has received (FDA) approval. • There is variable absorption of this medication, and adjustment of dose may be necessary.
Combination OCPs • Ethynodioldiacetate: • a progestin of low androgenic potential, • is combined with ethinyl estradiol: 35 or 50 mcg (in Zovia® 1/35-28 or 1/50-28, respectively). • The 1/50 preparation is useful for patients who require a large dose of estrogen, such as those with obesity or dysfunctional uterine bleeding.
Combination OCPs • After three months, • the efficacy of treatment is assessed by evaluating clinical symptoms and androgen levels. • If the treatment is effective, as a general rule, OCPs should be continued until the patient is gynecologically mature (five years postmenarcheal) or has lost a substantial amount of excess weight. • At that point, withholding treatment for a few months to allow recovery of suppression of pituitary-gonadal function and to ascertain whether the menstrual abnormality is persistent is advisable. • In doing so, however, one must keep in mind that the anovulatory cycles of PCOS lead to relative infertility, not absolute infertility.
Combination OCPs • If treatment is not successful in reducing androgen levels, • the patient either has an unusually prominent component of functional adrenal hyperandrogenism to the PCOS, OR • the diagnosis of PCOS should be questioned.
Combination OCPs • Limitations : The role of OCPs in the management of PCOS in adolescents may be limited for several reasons: • may make weight loss more difficult to attain because it promotes salt and water retention. • OCPs do not permit conception if and when it is desired. • In perimenarcheal girls with short stature who have open epiphyses, OCPs are contraindicated because OCPs contain growth-inhibitory amounts of estrogen. • Concerns have been raised that the incompletely mature adolescent neuroendocrine system may have heightened risk for post-pill amenorrhea and infertility [6]. However, this hypothetical concern is based on observations in other patient groups undergoing treatment with high-dose estrogens during adolescence, and its relevance to girls with PCOS is unclear. • Oestrogen treatment to reduce the adult height of tall girls: long-term effects on fertility, Lancet. 2004, Menzies Research Institute, University of Tasmania, Private Bag 23, Hobart 7001, Australia
Combination OCPs • Other risks of OCPs are similar in adolescents with PCOS to those without PCOS. • There is a risk of venous thromboembolism with use of OCPs that is primarily related to the dose and duration of estrogen use, although third generation progestins such as drospirenone confer about a twofold independent risk for first-time users . • Risk of non-fatal venous thromboembolism in women using oral contraceptives containing drospirenone compared with women using oral contraceptives containing levonorgestrel: case-control study using United States claims data, BMJ. 2011, Boston Collaborative Drug Surveillance Program, Boston University , USA. • Hormonal contraception and risk of venous thromboembolism: national follow-up study, BMJ. 2009, Gynaecological Clinic, Rigshospitalet, Copenhagen University, Denmark.
Progestin • Menstrual irregularities in sexually mature adolescents often can be controlled with cyclic progestin alone. • Transient reduction in androgen levels is variably achieved during cyclic therapy, but this is insufficient to expect improvement in hirsutism or hirsutism equivalents . • Effect of oral micronized progesterone on androgen levels in women with polycystic ovary syndrome, FertilSteril. 2002, Department of Obstetrics and Gynecology The University of Alabama at Birmingham, USA.
Progestin • Micronized progesterone (Prometrium®, 100 to 200 mg given orally at bedtime) or • medroxyprogesterone acetate (Provera®, 10 mg given orally at bedtime) can be used for 7 to 10 days out of each month or cycle.
Glucocorticoid therapy • There is considerable controversy about the efficacy and safety of glucocorticoid therapy for PCOS . • Glucocorticoid therapy does not result in consistent ovulation in patients with PCOS, even in those with a prominent component of functional adrenal hyperandrogenism . • Ovulation after glucocorticoid suppression of adrenal androgens in the polycystic ovary syndrome is not predicted by the basal dehydroepiandrosterone sulfate level, J Clin Endocrinol Metab. 1999, Department of Obstetrics/Gynecology, The University of Alabama at Birmingham, USA
GnRH agonists • used rarely in lieu of OCPs to regulate menstrual cyclicity or suppress ovarian function in the unusual patient who cannot tolerate OCPs and for whom progestins do not suffice. • GnRH therapy is generally not recommended in adolescents younger than 16 years of age because of concerns regarding bone mineral accrual.