Download
1 / 23
230 likes | 372 Views
3Cs & HIV Programme Chlamydia, Contraception, Condoms & HIV. A programme to support basic sexual health provision in general practice. 3Cs & HIV programme Supporting sexual health provision in general practice. The 3Cs & HIV programme is designed to support general practices deliver:

E N D
3Cs & HIV Programme Chlamydia, Contraception, Condoms & HIV A programme to support basic sexual health provision in general practice
3Cs & HIV programmeSupporting sexual health provision in general practice • The 3Cs & HIV programme is designed to support general practices deliver: • A basic sexual health offer (‘3Cs’) during any routine consultation with young adults (15 – 24 year olds): • A chlamydia screen • Signposting or provision of contraception advice • Free condoms • HIV testing in adults (≥ 16 years) in line with current clinical guidelines: • Awareness of indicator conditions where HIV testing should be considered • In high prevalence areas, routine offer of HIV test to all new practice registrants • The 3Cs & HIV programme is specifically designed meet the needs of, and to fit alongside work already being undertaken by, GP teams.
General practiceAn important role in sexual health promotion At least 60% of young adults visit their GP every year - and want the option of accessing sexual health services1,2 Most people become sexually active between 16-19 years old:3,4,5 Sexual activity can be opportunistic, unplanned and linked with alcohol and drugs STI rates and under 18 conceptions are indicators of ongoing health inequality 70% of young adults who have had a chlamydia test are more likely to test again in future, and 68% are more likely to recommend testing to friends The 3Cs & HIV programme will help young adults access sexual health advice and services to avoid negative health outcomes that may impact their future life chances • Salisbury et al. British Journal of General Practice. 2006; 56:99-103; 2. Hogan et al. BMC. Public Health 2010, 10:616; 3. DH. Improving Access to Sexual Health Services for Young People.2007 ; 4. DfES. Teenage Pregnancy Next Steps. 2006; 5. HPA Web Survey of Young Adults (2012)
HIV in the UK, 2011:1 Estimated 96,000 people living with HIV – 24% (22,600) are unaware of their infection Estimated prevalence of 1.5 per 1,000 population – higher among MSM and black Africans 47% of HIV cases diagnosed late (CD4<350) in 2011 Why focus on reducing late HIV diagnoses? Public health impact – treatment can prevent onward transmission2 - indicator within Public Health Outcome Framework Individual prognosis -early diagnosis can lead to near-normal life expectancy3 Cost -expanded HIV testing shown to be cost effective4-5and increased costs of a late versus early diagnosis (x2-3 times) which persist longer term7,8 3Cs & HIV programmeWhy include HIV testing? 1. HPA HIV in the UK 2012 report; 2. Cohen et al NEJM 2011 3. Nakagawa et al AIDS 2012; 4. Paltielet al N Engl J Med 2006; 5. Yazadanpanahet al Plos One 2011; 6. MMWR 2006; 7. Krentzet al HIV Med 2008; 8. Beck et al Plos One 2011
HIV testing: an opportunity in general practice 76% of people diagnosed with HIV had been seen in health services in previous year – of which, 76% in general practice1 Department of Health pilot projects investigated expanded HIV testing in general medical services:2 Feasible Cost-effective Acceptable to patients • Burns et al AIDS 2008 • HPA Time to Test for HIV Report 2011
3Cs &HIV programmeAnticipated results The 3Cs & HIV programme adapts an intervention trialled by the HPA to increase chlamydia testing in general practice In this randomised controlled trial, surgeries that fully engaged with the intervention significantly improved screening rates and chlamydia detection1 These results provide a realistic measure of the take up and efficacy of the 3Cs & HIV intervention if commissioned in General Practice The 3Cs & HIV programme is designed to strengthen sexual health work already funded and underway in your area, and support delivery of Public Health Outcomes Framework indicators • McNulty C. In press
3Cs & HIV programmeOutline of delivery • The 3Cs & HIV programme is designed to fit into current general practice activity, and support surgeries engage young adults in an evidence-based sexual health intervention • The NCSP will offer 1,500 surgeries across England the opportunity to participate in 2013/14: • Local areas sign up to participate and identify a local 3Cs & HIV trainer • NCSP ‘train the trainers’ and provide all 3Cs & HIV programme materials • 3Cs trainers engage local practices in participating • Local 3Cs & HIV practices deliver offer to young adults on ongoing basis • 3Cs & HIV practice data collected and evaluated across 2013/14
8 An evidence-based programme Employing the Theory of Planned Behaviour
The Theory of Planned Behaviour Personal Attitudes Subjective Norms Intention to Screen Behaviour: sexual health offer for all young adults Perceived Barriers External Barriers Chlamydia screen offer forgotten, surgery premises’ barriers etc.
Theory of Planned Behaviour: supporting general practice engage young adults in chlamydia screening IDENTIFIED BARRIERS INTERVENTION SOLUTION “Low numbers of young adults visit my practice” Personal Attitudes Show surgery annual footfall for 15-24 yr olds Discuss the evidence base showing young adults’ preference for sexual health services via their GP “Young adults don’t want to talk about sexual health” “My colleagues do not offer sexual health care to young adults” • Normalise the sexual health offer through: • Appointing a sexual health champion per surgery • Surgery posters promoting the initiative • Invite cards given to young adults at Reception Subjective Norms “I lack knowledge about STIs, HIV and pregnancy rates” Practice staff offered training sessions and provided with information resources Perceived Barriers “I lack experience / confidence engaging young adults in sexual health matters” Training videos show the offer being delivered
External barriers The use of computer pop ups & templates encouraged Forgetting to make the offer during a routine consultation GP practice receives three contacts, including at least one visit Risk that practice momentum declines over time GP practice receives regular newsletter and information on the practice’s results Intervention can be tailored to suit each surgery’s set up Practice environment not conducive to making the offer
South West of England Trial Results1 • Analysed 76 intervention and 81 control surgeries. Of the 76 surgeries offered the intervention: • 47 (63%) fully engaged (received three contacts with support worker) • 16 (21%) partially engaged (received one or two contacts) • 13 (17%) did not engage (refused all contacts) • During the trial period: • 2,907 vs. 2,379 screens in intervention and control surgeries, respectively • 76% screening increase in intervention surgeries vs. controls (p<0.001) • 40% increase in infections detected per surgery population (p=0.04) • ‘Fully engaged’ intervention surgeries: • Increased screening rates 2.33 times vs. controls (p<0.001) • Increased chlamydia detection by 76% (p=0.005) • Increased screening significantly for at least 9 months following the intervention • McNulty C. In press
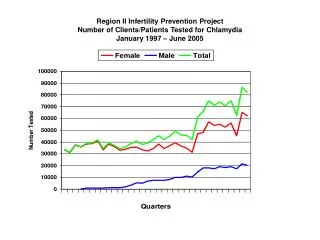
South West of England Trial Results1 Increase in screening is sustained nine months after support endedin intervention practices Once trained, 3Cs & HIV surgeries can use programme to strengthen their sexual health offer on long-term basis Start of intervention Support ends Impact sustained Intervention period Chlamydia screening rate per 100 15-24 year olds in study surgeries January 2009 to January 2012, by month • McNulty C. In press
South West of England Trial:Qualitative Results • Feedback from qualitative interviews: • Intervention was detailed and thorough • Easy access to the support available • Chlamydia support team went to the surgery to implement the intervention • Chlamydia support team stayed in contact over a year • Reward and recognition “I think probably coming and actually explaining what it was and giving us the support and phone support after and coming back to the practice and checking how we were doing was helpful” Practice Nurse
3Cs & HIV programme development:Preliminary GP interviews “I think GU services and contraception go hand in hand” “I think doing all ‘three Cs’ would be reasonable” “It’s a good idea to make the link between chlamydia, condoms and contraception. It makes sense to look at prevention at the same time as cure” “We should be giving sexual health advice alongside the chlamydia testing, otherwise we’re just testing not educating” “Really, I think it’s vital that chlamydia testing is offered with these other things as well” “It’s a population that needs a bit of lateral thinking on how to engage them”
16 3Cs & HIV programme delivery
3Cs & HIV programme: Local area participation • NCSP currently inviting expressions of interest from areas • To participate, areas must identify someone currently working in sexual health to become their 3Cs & HIV trainer • The 3Cs & HIV trainer will deliver the programme locally: engaging local practices, providing ongoing support and evaluating achievements • The time required by 3Cs & HIV trainers will vary per area, depending on the number of practices engaged, but estimated at 0.5 WTE if 30 practices
3Cs & HIV programme: NCSP role • ‘Train the 3Cs & HIV trainer’ course • Two follow up contacts with each 3Cs & HIV trainer • 3Cs & HIV resource pack for practices • Free condoms • Performance data, per practice • Project coordination and monitoring The NCSP will provide the following to support local delivery of the 3Cs & HIV programme:
3Cs & HIV programme:Support and resources for practices The programme is designed by GPs to fit general practice – and can be tailored to each practice, building on their current skills and services. Each practice receives: • An interactive training session • Ongoing supportive follow up from their area trainer • 3Cs & HIV practice resources to promote the programme • 3Cs & HIV website – further information and resources
3Cs & HIV data collection • The NCSP will evaluate the impact of the 3Cs & HIV programme • Using local systems to collect data by practice on: • Chlamydia testing and diagnoses • Contraceptive prescribing data for 15-24 year olds • HIV testing • Registration / use of C-card and local condom programmes • Aim: data available ~6 months after the end of each quarter
Timeline Jan – May 2013: expressions of interest & participant selection May – Jun 2013: NCSP training of 3Cs local area trainers End of May – Jul 2013: 3Cs & HIV trainers recruiting GP surgeries Jul 2013 onwards: 3Cs & HIV programme delivery roll out
What next? • If you are interested in participating, please discuss with your NCSP sexual health facilitator: • London meroe.bleasdille@phe.gov.uk • South East & Central ruth.e.hall@phe.gov.uk • East of England wendy.elliott@phe.gov.uk • West Midlands janet.deeming@phe.gov.uk • North West patrick.lenehan@phe.gov.uk • Yorkshire, Humber & North East sharron.ainslie@phe.gov.uk • East Midlands deborah.shaw@phe.gov.uk • South West norah.obrien@phe.gov.uk • We look forward to working with you.
3Cs & HIV Programme Chlamydia, Contraception, Condoms & HIV