Download
1 / 55
580 likes | 824 Views
TNM staging system for Renal Cell Carcinoma: current status and future perspectives. Vincenzo Ficarra Dipartimento di Scienze Oncologiche e Chirurgiche Clinica di Urologia - Università degli Studi di Padova. Staging systems for RCC. An ideal cancer staging system should effectively:

E N D
TNM staging system for Renal Cell Carcinoma: current status and future perspectives Vincenzo Ficarra Dipartimento di Scienze Oncologiche e Chirurgiche Clinica di Urologia - Università degli Studi di Padova
Staging systems for RCC • An ideal cancer staging system should effectively: • comunicate critical tumor characteristics, • aid the clinician in the appropriate selection • of therapeutic options, • stratify the patient’s risk of cancer progression • or cancer death and • eventually determine the selection criteria for • clinical trials Sobin LH: TNM classification of malignant tumours; 2002
Staging systems for RCC • Flocks and Kadesky, 1958 • Robson, 1969 • TNM, 1978 • TNM, 1987 • TNM, 1997 • TNM, 2002 • TNM, ….. ?
Development of the TNM staging system for localized RCC Ficarra V.et al. Eur Urol 2004; 46: 559-64
Hafez KS et al. J. Urol. 1999; 162: 1930-1933 TNM, 2002 Version – Why ? • This update was mainly proposed to help the clinicians • to identify patients suitable for a elective partial nephrectomy
Radical nephrectomy Vs partial nephrectomy: comparative, non randomized studies Patients with RCC 4 cm (pT1a)
pT1a pT1b pT2 pT1a Vs pT1b (p = 0.0001) pT1a Vs pT2 (p < 0.0001) pT1b Vs pT2 (p = 0.0002) Multi-Institutional European Validational of the 2002 TNM Staging System • 2,217 localized RCC • 10-year CSS (%): • pT1a: 91% • pT1b: 83% • pT2: 75% Ficarra V. et al. Cancer 2005; 104: 968-74
BUT … is this the best strategy to subdivide confined RCC ? Patard JJ, Ficarra V et al. J. Urol 2004; 171: 2181-2185
Elective Partial Nephrectomy for pT1b RCC Bensalah K. et al. Eur. Urol 2008; 53: 691-693
Anatomic features related toselection of the candidate for NSS • Peripheral or • intraparenchymal location • Spherical shape • Adiacent nodular areas • Tumor deepening into the kidney • Relathionship with UCS Ficarra V et al. Eur Urol 2008 (in press)
BUT … is this the best strategy to subdivide confined RCC ? Identification of different risk groups for progression or death • 4.5 cm (Zisman, 2001) • 5 cm (Gelb, 1993; Targaski, 1994; Igarashi,2001; • Lau, 2002; Elmore, 2003; Zucchi, 2003) • 5.5 cm (Kinouchi, 1999; Ficarra, 2004) Ficarra V et al. Eur. Urol 2004; 46: 559-564
Proposal for Revision of the TNM 1,138 patients with a mean follow-up of 87 months after partial or radical nephrectomy 5.5 cm Ficarra V., Patard JJ et al Cancer 2005; 15: 104: 2116-23
Proposal for Revision of the TNM Staging System for Renal Cell Carcinoma Ficarra V. et al Cancer 2005; 15: 104: 2116-23
Prognostic Stratification of Localized Renal Cell Carcinoma by Tumor Size 464 patients with a mean follow-up of 60 months after radical or partial nephrectomy Bedke J. et al J Urol 2008; 180: 62-67
Prognostic Stratification of Localized Renal Cell Carcinoma by Tumor Size 5.5 cm 7 cm Bedke J. et al J Urol 2008; 180: 62-67
Proposal for Revision of the TNM • Ficarra et al, 2005 • Multicenter study (7 Centres) • 1984 - 2001 • Retrospective • 1,138 cases • - 873 RN • - 265 NSS • Median tumor size: 5 cm • IQR tumor size: 3-7 cm • Median FU: 87 mo • (IQR FU: 68-130 mo) • Martingale residuals: 5.5 cm • Cut-off: 5.5 cm • Bedke et al, 2008 • Single Center study • 1990 - 2006 • (?) Prospective • 464 cases • - 398 RN • - 66 NSS • Median tumor size: ? • IQR tumor size: ? • Median FU: 60 mo • (range FU: 1-180 mo) • Martingale residuals: 5.5 cm • Cut-off: 7 cm
Prognostic Impact of Tumor Size on pT2 706 patients with pT2 RCC surgically treated at 9 International academic centers Klatte T., Patard JJ, Ficarra V., et al J Urol 2007; 178: 35-40
Tumor Size Improves the Accuracy of TNM Predictions in patients with Renal Cancer • Identification of an ideal breakpoint represents • a complex process, wich is affected by differences • in patient characteristics • Spectrum bias and associated floor and ceiling • effects may be circumvented, if variables are • used without being catagorized Karakiewicz PI, Ficarra V. Patard JJ et al Eur Urol 2006; 50: 521-529
Tumor Size Improves the Accuracy of TNM Predictions in patients with Renal Cancer Karakiewicz PI, Ficarra V. Patard JJ et al Eur Urol 2006; 50: 521-529
AJCC/UICC stage groupings cannot Incorparate countinuosly coded variables Karakiewicz PI, Ficarra V. Patard JJ et al JCO 2007; 25: 1316-1322
Development of the TNM staging system for locally advanced RCC TNM, 1987 TNM, 1997 TNM, 2002 T3a Fat and adrenal inv. Fat and adrenal invasion T3b Renal vein (V1) V1 – V2 T3c IVC below diaphr (V2) V3 T4 Outside Gerota’s fascia T4a Outside Gerota’s fascia T4b IVC above diaphr (V3).
Multi-Institutional European Validational of the 2002 TNM Staging System 1,969 locally advanced (pT3-4) RCC • pT3a: Fat and/or • adrenal invasion • pT3b: renal vein or IVC • below diaphr. • pT3c: IVC above diaphr. • pT4: beyond Gerota 60% pT3a 46% pT3b 12% pT3c p value < 0.0001 pT4 Ficarra V., et al. J Urol 2007; 178: 418-424
1,117 pT3a RCC Perirenal fat Adrenal only p value = 0.0002 New staging system for pT3-4 RCC: a multicentric european study Ficarra V., et al. J Urol 2007; 178: 418-424
705 pT3b RCC V1 V1+fat V2 V2+fat p value< 0.0001 V1-2+adrenal New staging system for pT3-4 RCC: a multicentric european study Ficarra V., et al. J Urol 2007; 178: 418-424
Reclassification of patients with pT3 and pT4 RCC improves prognostic accuracy Thompson RH et al. Cancer 2005; 104: 53-60
Reclassification of patients with pT3 and pT4 RCC improves prognostic accuracy Thompson RH et al. Cancer 2005; 104: 53-60
Proposal for reclassification of the TNM In patients with pT3-4 RCC pT3a = perirenal fat invasion or renal vein involvement (V1) or IVC below diaphragm (V2) pT3a new pT3b: V1 or V2 plus concomitant perirenal fat invasion pT3b new pT4 new pT4: adrenal gland or Gerota fascia invasion or IVC above diaphragm (V3) p < 0.001 Ficarra V et al. Eur Urol 2007; 51: 722-731
Redefining pT3 Renal Cell Carcinoma In the modern Era Margulis V. et al. Cancer 2007; 109: 2439-44
New staging system for pT3-4 RCC: a multicentric european study Ficarra V., et al. J Urol 2007; 178: 418-424
New staging system for pT3-4 RCC: a multicentric european study 1,969 pT3-4 RCC 1,248 pT3-4 N0M0 RCC pT3a (new) pT3a (new) pT3b (new) pT3b (new) pT4 (new) pT4 (new) p value< 0.0001 p value< 0.0001 Ficarra V., et al. J Urol 2007; 178: 418-424
New staging system for pT3-4 RCC: a multicentric european study Ficarra V., et al. J Urol 2007; 178: 418-424
Renal sinus involvement in RCC Bonsib SM et al. Am J Surg Pathol 2000; 24: 451-458
Renal sinus involvement in RCC Thompson RH et al. J Urol 2005; 174: 1218-1221
Renal sinus involvement in RCC 365 patiens with pT3a RCC Margulis V et al. J Urol 2007; 178: 1878-1882
Renal sinus involvement in pT3a
Prognostic relevance of tumour size in T3a 623 patients with pT3a Renal Cell Carcinoma Lam JS., Ficarra V, Patard JJ et al. Eur Urol 2007; 52: 155-162
Prognostic relevance of tumour size in T3a N0 / M0 N0-2 / M0-1 Lam JS., Ficarra V, Patard JJ et al. Eur Urol 2007; 52: 155-162
Urinary collecting system invasion • Urinary collecting system (UCS) involvement is not • included in the current TNM staging system. • The UCS invasion in high stage tumours did not support a significantly worse prognosis, whereas in low stage tumours this prognostic factor can influence negatively the cancer specific survival rate • However, in published series the UCS invasion did not result an independent prognostic factor • At this time, this pathologic finding should not be considered in the new TNM staging system.
Proposal of an improved prognostic Classification for pT3 Terrone C. et al. J Urol 2008; 180: 72-78
Proposal of an improved prognostic Classification for pT3 Terrone C. et al. J Urol 2008; 180: 72-78
New staging system for pT3-4 RCC: a multicentric european study 1,969 pT3-4 RCC pT3a (new) 645 (524) pT3b (new) 241 (223) pT4 (new) 159 (156) p value< 0.0001 Ficarra V., et al. J Urol 2007; 178: 418-424
A new staging system for locally advanced (T3-4) RCC Ficarra V et al. Eur Urol 2007; 51: 722-729
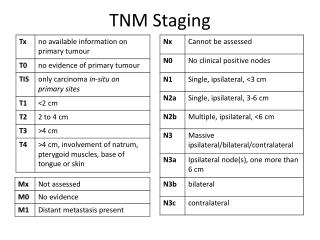
Tumour Nodes and Metastases (TNM) Staging System TNM, 1987 TNM, 1997 TNM, 2002 Nx Regional Lymph nodes idem idem cannot be assessed N1 Metastasis in 1 Lymph Metastasis to Metastasis to node 2 cm a single node a single node N2 Metastasis in 1 Lymph Metastasis in > Metastasis in > node > 2 cm but < 5 cm 1 Lymph node 1 Lymph node N3 Metastasis in 1 Lymph node > 5 cm
Reassessing the current TNM Lymph Node Staging for RCC Terrone C et al. Eur Urol 2006; 49: 324-331
Reassessing the current TNM Lymph Node Staging for RCC Terrone C et al. Eur Urol 2006; 49: 324-331
Reassessing the current TNM Lymph Node Staging for RCC Dimashkieh HH et al. J Urol 2006; 176: 1978-1983
Cancer-specific survival according to TNM Staging System 39% 30% (4.3%) 27% 15% 8% Karakiewicz P., Ficarra V. et al. Eur Urol 2007; 51: 1616-24
Other Independent Prognostic Factors • Age at diagnosis, mode of presentation, • performance status ECOG • Pathological tumour size, Nuclear grading, • Tumour necrosis, Sarcomatoid differentiation • (?) Tumour histological type • Molecular and genetic variables