Download
1 / 28
290 likes | 655 Views
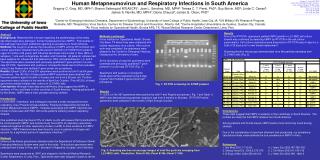
Human Metapneumovirus and Lower Respiratory Tract Disease in Otherwise Healthy Infants and Children The NEW ENGLAND JOURNAL OF MEDICINE JANUARY 29,2004. ABSTRACT.

E N D
Human Metapneumovirus and Lower Respiratory Tract Disease in Otherwise Healthy Infants and ChildrenThe NEW ENGLAND JOURNAL OF MEDICINEJANUARY 29,2004
ABSTRACT • .Respiratory syncytial virus (RSV), parainfluenza virus, adenovirus,and influenzavirus are common known causes of lower respiratorytract disease in infants and children.Nevertheless, ina substantial portion of lower respiratory tract infectionsin children, no virus can be cultured. In 2001, researchersin the Netherlands isolated a new virus from children and adultswith acute respiratory tract infection.
This RNA virus, provisionallydesignated human metapneumovirus, is closely related to avianpneumovirus. Since then, investigators in Canada, Australia,the United Kingdom, and the United States have described patientswith acute respiratory tract infection due to human metapneumovirus.
e sought to determine the role of human metapneumovirusin lower respiratory tract illness in previously healthy infantsand children
Methods • We tested nasal-wash specimens, obtained over a 25-yearperiod from otherwise healthy children presenting with acuterespiratory tract illness, for human metapneumovirus • Children in whomchronic diseases developed, other than mild asthma, were excluded
During visits for illness,the children's signs and symptoms were recorded on a standardizedclinical form, the information was reviewed and entered intoa data base, and nasal-wash samples were obtained and culturedfor viruses.
Case Definitions • The clinician made the diagnosis at the time of the child'svisit. Wheezing, rales, tachypnea, and dyspnea were consideredto be signs of lower respiratory tract infection. Bronchiolitiswas defined as an acute respiratory illness characterized byrhinorrhea, cough, and diffuse wheezes and rales, with peribronchialthickening and hyperexpansion on the chest radiograph, if onewas obtained..
Pneumonia was defined as dyspnea in a patientwith focal rales or decreased breath sounds and the presenceof a focal infiltrate on the chest radiograph. Laryngotracheobronchitis(croup) was defined as an acute lower respiratory tract infectioncharacterized by hoarseness, cough, and stridorNasal-washspecimens for viral culture were obtained from children withany of the following indications: an upper respiratory tractinfection accompanied by a temperature greater than 38.4°C,acute otitis media, or evidence of a lower respiratory tractinfection.
Culture of Human Metapneumovirus Isolates • . Wells with a cytopathiceffect, consisting of rounded cells and focal plaques, weretested for the presence of human metapneumovirus by RT-PCR.Cultures without a cytopathic effect were passaged onto freshcell monolayers after 14 days and incubated for an additional14 days.
RESULTS • Seventeen percent of the child-years were accounted for by infantsyounger than 6 months of age, 15 percent by children 6 to 12months of age, 25 percent by children 13 to 24 months of age,19 percent by children 25 months to 3 years of age, and 24 percentby children older than 3 years of age. Fifty-one percent ofthe infants enrolled were male, 53 percent were white, and 44percent were black. • A total of 1127 visits were associated with the diagnosis oflower respiratory tract infection;
Lower Respiratory Tract Infection with Human Metapneumovirus • Forty-nine of the 248 tested samples (20 percent) were positivefor human metapneumovirus by RT-PCR\ • . Of the 49 samples that were positive for human metapneumovirus,3 were also positive for RSV on RT-PCR, for a coinfection rateof 6 percent. Specimens from 96 patients with lower respiratorytract infection who had previously had positive cultures forother viruses were tested for human metapneumovirus by RT-PCR.Four were also positive for human metapneumovirus, yieldinga coinfection rate for these samples of 4 percent
There wasno apparent difference in the severity of disease between childrenwith coinfections and those infected with human metapneumovirusalone. Of 86 nasal-wash specimens from children without respiratorysymptoms that were tested, only 1 was positive for human metapneumovirus.
The male:female ratio among patients with lower respiratorytract infection due to human metapneumovirus was 1.8:1, witha mean age of 11.6 months, a median age of 6.5 months, and anage range of 1.5 to 50 months. Lower respiratory tract infectionwith human metapneumovirus occurred predominantly in the firstyear of life, and the age distribution thus differed from thatof the clinic population: 25 percent of human metapneumovirusinfections occurred among infants under six months of age, and49 percent occurred among infants six months to one year ofage.
. Epidemiologic Pattern of Lower Respiratory Tract Infections with Human Metapneumovirus and Other Viruses
The clinical diagnosis given to the 49 children with human metapneumovirusinfection of the lower respiratory tract was bronchiolitis in29 (59 percent), croup in 9 (18 percent), pneumonia in 4 (8percent), and an exacerbation of asthma in 7 (14 percent) (Table 2).Acute otitis media was diagnosed in 18 (37 percent). Fourteenchildren underwent chest radiography, and the results were abnormalin seven (50 percent), with the radiographs in most of thesechildren showing diffuse perihilar infiltrates (Figure 3). Oneof the 49 children (2 percent), who was 36 months of age, washospitalized with the diagnosis of an exacerbation of asthmatriggered by a viral respiratory tract infection.
Comparison with Other Viral Infections • . Fever occurred less often with human metapneumovirusinfection than with influenzavirus infection (52 percent vs.87 percent, P=0.001) but at a rate similar to that for infectionswith RSV, parainfluenza virus, or adenovirus. Vomiting occurredless often with human metapneumovirus infection than with RSVinfection (in 10 percent of children vs. 31 percent, or influenzavirus infection (10 percent vs. 28 percent,
On physical examination, rales and wheezing were noted lessoften in children with human metapneumovirus infection thanin those with RSV infection (8 percent vs. 24 percent, P=0.03,and 52 percent vs. 69 percent, P=0.04, respectively), but ata rate similar to that for parainfluenza virus, influenzavirus,or adenovirus infection. Conjunctivitis was noted less frequentlywith human metapneumovirus infection than with influenzavirusinfection (4 percent vs. 22 percent, P=0.02), whereas the ratesof rhinitis and rhonchi were similar among the viruses.
The distribution of specific clinical syndromes caused by humanmetapneumovirus differed from that of the other viruses (Table 2).Human metapneumovirus infection was more likely to be associatedwith clinical bronchiolitis and less likely to be associatedwith croup than was infection with parainfluenza virus or influenzavirus.Human metapneumovirus infection was less likely to be associatedwith pneumonia than was infection with RSV or influenzavirus.There was an association between human metapneumovirus infectionand the diagnosis of an exacerbation of asthma
Upper Respiratory Tract Infection with Human Metapneumovirus • 15percent) were positive for human metapneumovirus. The seasonaldistribution of the onset of illness in these patients was similarto that among patients with lower respiratory tract infectioncaused by human metapneumovirus,.
whereas the mean age was 19.6months — older than that of patients with lower respiratorytract infection caused by human metapneumovirus) butnot significantly different from the mean age of all patientswith upper respiratory tract infections The male:femaleratio among patients with upper respiratory tract infectioncaused by human metapneumovirus was 0.9:1
Recurrent Infection with Human Metapneumovirus • Three patients had evidence of recurrent infection with humanmetapneumovirus A boy was given a diagnosis of bronchiolitisat 3.5 months of age and of upper respiratory tract infectionat 42 months of age, a girl received a diagnosis of bronchiolitisat 4.5 months of age and of upper respiratory tract infectionat 19 months of age, and another girl had an upper respiratorytract infection at both 6 months and 32 months of age
CONCLUSIONS • Human metapneumovirus infection is a leading causeof respiratory tract infection in the first years of life, witha spectrum of disease similar to that of respiratory syncytialvirus.
Human metapneumovirus was presentin 20 percent of all cases of lower respiratory tract infectionwithout a prior virologic diagnosis. • Three quarters of all lower respiratorytract infections caused by human metapneumovirus occurred inthe first year of life
Disease due to human metapneumovirusoccurred in late winter • We also found human metapneumovirus in 15 percent of patientswith upper respiratory tract infections
there is a strong associationbetween human metapneumovirus and lower respiratory tract infectionin otherwise healthy children and that human metapneumovirusis a major cause of bronchiolitis and croup in the pediatricpopulation. Lower respiratory tract infections occurred predominantly in the first year of life, during the late winter months.Thehospitalization rate was similar to that for RSV infection,and otitis media was a frequent complication