Download
1 / 98
1.1k likes | 1.68k Views
Rehan A Khan, M.D. Staff Gastroenterologist John D. Dingell VAMC Detroit, MI. Pancreatic Diseases. Anatomy of the Pancreas. The pancreas is a soft, elongated, and flattened gland of 12 to 20 cm in length and weighs between 70 and 110 g

E N D
Rehan A Khan, M.D. Staff Gastroenterologist John D. Dingell VAMC Detroit, MI Pancreatic Diseases
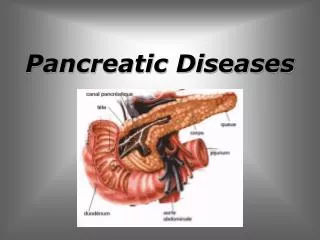
Anatomy of the Pancreas The pancreas is a soft, elongated, and flattened gland of 12 to 20 cm in length and weighs between 70 and 110 g The head of pancreas is retroperitoneal and found posterior to the stomach and lesser omentum It is lobular in appearance The neck, body, and tail of the pancreas lie obliquely in the posterior abdomen, with the tail extending as far as the gastric surface of the spleen
Anatomy of the Pancreas HEAD OF THE PANCREAS The second and third duodenum curvatures lie around the head of the pancreas The anterior surface is adjacent to the pylorus, the first part of the duodenum, and the transverse colon UNCINATE PROCESS Projects off the lower part of the head of the pancreas It lies anterior to the aorta and inferior vena cava and is covered superiorly by the superior mesenteric vessels
Anatomy of the Pancreas NECK OF THE PANCREAS It is 1.5 to 2.0 cm long and 3.0 to 4.0 cm wide Anteriorly, it is covered in part by the pylorus and peritoneum of the lesser sac Posteriorly, lies the confluence of the portal vein with the superior mesenteric and splenic veins BODY OF THE PANCREAS Anterior to the body are antrum, body of the stomach and the transverse mesocolon Posterior to the body are the aorta, the origin of the superior mesenteric artery and the splenic vein The midline part of the body overlies the lumbar spine, which makes this area of the pancreas most vulnerable to abdominal trauma
Anatomy of the Pancreas TAIL OF THE PANCREAS Its tip usually reaching the hilus of the spleen The splenic artery and vein contained between the two layers of the splenorenal ligament
Circulation Arterial Supply Branches of the celiac and superior mesenteric arteries All major arteries lie posterior to the ducts Venous Drainage Venous drainage of the pancreas is similar to the arterial blood supply. It drains into the portal venous system- formed by joining of the superior mesenteric and splenic veins The splenic vein originates at the hilum of the spleen Pancreatic veins drain the neck, body, and tail of the pancreas and join the splenic vein
Lymphatic and Innervations Lymphatic Drainage Pancreatic cancer first metastasize to the regional lymph nodes Nerve Supply The visceral efferent innervations of the pancreas is through the VAGUS and SPLANCHNIC Nerves by way of the Hepatic and celiac plexuses
Pancreatic Cells Two distinct organ systems within the pancreas The Endocrine Glands Islet of Langerhans up to 20% of organ 1-2% of the pancreatic endocrine tumors Alpha cells-produce glucagon and constitute approximate 25% of the total islet cell number Beta cells-the Insulin producing cells (majority of the cells) Delta cells-produce Somatostatin (smallest number)
Pancreatic Cells The Exocrine Glands Made up of Acini and Ductal systems Three different epithelial cell types can be found in the normal pancreas ACINAR CELLS:Composed about 80% of organ Itsynthesizes, store and secretes digestive enzymes 5-10% of pancreatic tumor – Adenocarcinoma Duct Cells: Constitutes 10-20% of the organ Secretory function 85-90% of Pancreatic Tumor - Ductal Adenocarcinoma
Splenic Vein Thrombosis • Isolated Gastric Varices: Inflammatory or Neoplastic diseases involving the pancreatic body and tail can lead to splenic vein occlusion • Retrograde venous drainage toward the splenic hilum and then, by way of flow through the short gastric and left gastroepiploic veins, can create UGI bleed from GASTRIC VARICES
Normal anatomic relation of the pancreas with other intra-abdominal structures as shown by computed tomography. The borders of the pancreas are indicated by arrowheads. The splenic vein is indicated by an arrow. A, aorta; C, vena cava; G, incidental gallstone; I, small intestine; K, left kidney; L, liver; P, portal vein; S, stomach; V, vertebra. (Courtesy of M. P. Federle, MD.)
Physiology of Pancreas The pancreas normally secretes approximately 1.5 liters of enzyme-rich fluid every day for the digestion of fats, starch, and protein Fasting state Protein-rich with bicarbonate concentration of 80 mEq/L Post-Prandial A large volume of alkaline, enzyme-rich fluid enters the duodenum to neutralize gastric chyme for optimal digestion
Pancreatic Secretions Secretin Released from the duodenal mucosa in response to the presence of acid in the duodenum to maintain isotonicity Stimulates the release of bicarbonate and water from the interlobular duct cells (HCO3-120 meq/l) Reciprocal decrease in Cl CCK Released from the gut endocrine cells in response to the entry of fats and proteins into the proximal intestine Stimulates pancreatic acinar cells Release digestive proenzymes
Manifestation of Pancreatic insufficency Maldigestion of fat and proteins Steatorrhea- 90% of glandular function lost Weight Loss Fat soluble vitamin Deficiency (ADEK) Impaired night vision (A) Metabolic Bone Disease (D) B12 deficiency Decrease intestinal Ph may affect transfer of B12 from R protein to intrinsic factor
Acute Pancreatitis An acute inflammatory process of the pancreas (diagnostic-2 of 3 present) • Abdominal Pain • Elevated Amylase and Lipase • Abnormal Imaging (US abdomen or CT scan)
Pathology INTERSTITIAL nECROTIZING Extensive parenchymal destruction Peri-pancreatic fat necrosis Severe form High morbidity and mortality • Edema • Inflammation of pancreatic parenchyma • Clinically milder presentation
Etiologies of Acute Pancreatitis • Most Common Alcohol Gallstone Idiopathic (20 %) • Less CommonViral Infection Post ERCP Parasitic infestation of pancreatic duct Hyperlipidemia Hereditary Medications Hypercalcemia SOD Pancreatic Divisum
Clinical Presentation • Abdominal Pain Epigastric or LUQ-radiation to back, steady or infrequent, diffuse or localized or biliary colic • Nausea and vomiting • Fever • Hypotension • Tachycardia • Tachypnea
Physical Signs • SIRS or Sepsis or Septic shock or ARDS • Acute Abdomen • Localized tenderness with rebound tenderness • Cullen sign (periumblical echymoses) • Gray Turner Sign (flank echymoses) • Jaundice
Cullen’s Sign Cullen's sign is superficial edema and bruising in the subcutaneous fatty tissue around the umbilicus. This sign takes 24-48 hours to appear and can predict acute pancreatitis, with mortality rising from 8-10% to 40%.
Gray Turner Sign Grey Turner's sign refers to bruising of the flanks. Takes 24–48 hours. It can predict a severe attack of acute pancreatitis, with mortality rising from 8-10% to 40%. It is a sign of retroperitoneal hemorrhage. Causes: Acute Pancreatitis, blunt abdominal trauma, ruptured abdominal aortic aneurysm. Ruptured/ hemorrhagic ectopic pregnancy. spontaneous bleeding secondary to coagulopathy (congenital or acquired)
Laboratory Findings • Leukocytosis • Elevated Amylase (sensitive but less specific) • Elevated Lipase (more sensitive and specific) • Mostly 3 x ULN • Elevated Aminotranferases and Bilirubin level
Abdominal Imaging • US of RUQ/Gall Bladder • CT abdomen and Pelvis with IV contrast • MRI/MRCP abdomen • Repeat CT mostly after 3 days of admission or earlier if clinical deterioration (to evaluate necrosis) • If clinical improved-Don’t do further imaging
Criteria for Pancreatitis Not Due to Gallstones At admission During Initial 48 Hours Age over 55 years White blood count > 16,000 Blood glucose > 200 mg Serum lactate dehydrogenase (LDH) > 350 IU/L AST > 250 IU/L Hematocrit fall > 10 percentage points BUN elevation > 5 Serum calcium fall to < 8 Arterial oxygen concentration < 60 Base deficit > 4 Estimated fluid sequestration > 6L Early Prognostic Signs of Acute Pancreatitis- Ranson’s Criteria
Criteria for Gallstone Pancreatitis At Admission During Initial 48 Hours Age over 70 years White blood count > 18,000 Glucose > 220 Serum lactate dehydrogenase (LDH) > 350 IU/L AST > 250 IU/L Hematocrit fall > 10 percentage points BUN elevation > 2 Serum Calcium fall to < 8.0 Base deficit > 5 Estimated fluid sequestration > 4L Early Prognostic Signs of Acute Pancreatitis
The Atlantic Classification • Most widely used clinical systems • Differentiate b/w mild and severe form of disease • Criteria for Severity • Hypotensive Shock • Pulmonary Insufficiency (PaO2 < 60 mm Hg) • Renal failure • GI Bleeding (>500 ml/24 hr) • Pseudocyst, abscess or pancreatic necrosis • Three or more Ranson’s criteria • 8 or more APACHI II criteria
The Atlantic Classification • Goal standard for predicting severity of acute pancreatitis is CRP 150 mg/L • Hemoconcentration off 44 or more at admission • IL-6 • IL-8 • Procalcitonin • Serum Trypsinogen activation peptides • Polymorphonuclear Elastase • Carboxypeptidase Activation Peptide
Treatment of Interstitial Acute Pancreatitis • Admit to General ward • IV fluids • Analgesics • Nutrition-Vital NO NPO NO TPN Oral or Enteral feedings • NO prophylactic antibiotic • No need for follow-up imaging • Gallstone pancreatitis-Cholecystectomy before discharged-should have intra operative cholangiogram • Poor surgical candidate-ERCP with biliary sphincteromy
Treatment of Acute Necrotizing pancreatitis • Admit to ICU or telemetry • Supportive care with aggressive IV hydration • Prevention of Infection • Prevention of potential complications • High mortality during first two weeks (almost 100%) due to multiorgan failure, ARDS, ARF, Coagulopathy, shock, hypocalcaemia and hyperglycemia
Antibiotics • Infected necrosis in 30-70% • About 80% of death due to infection • Selective gut decontamination against gram negative bacteria-protect against colonic bacterial translocation • Imipenem-cilastatin (Primaxin) • Quinolone (reduce infection but not mortality) • Meropenem
Nutrition • Enteral nutrition is associated with Lower incidence of infection • Reduced numbers of surgical intervention to control pancreatitis • Decreased length of hospital stay • Patient with Ileus- No Enteral feeding
Surgical Intervention • Sterile pancreatic necrosis-no surgery since mortality is around 10% • Infected acute pancreatic necrosis-surgical intervention-Pancreatectomy (at least 30% late mortality)
Chronic Pancreatitis • Chronic pancreatitis (CP) is a progressive inflammatory disease of the pancreas resulting in slow destruction of pancreatic parenchyma and subsequent fibrosis
Alcoholic Idiopathic (10-20%) Tropical Inherited (CF) Traumatic Autoimmune Metabolic Hypertriglyceridemia Hypercalcemia OBSTRUCTIVE Benign obstructive SOD Papillary stenosis Pancreas divisum Neoplastic obstruction Tumors of ampulla or ductal system Etiologies Wolfe, MM. Educational Review Manual in Gastroenterology2004
Clinical Features • Pain • Maldigestion • Diabetes
Abdominal Pain • Cardinal feature of presentation in 90% of patients with CP • The most common indication for surgical intervention in patients with CP • The pain is typically epigastric, often radiates to the back, and is occasionally associated with nausea and vomiting. Often worse post prandial and may be relieved by sitting upright or leaning forward • Two types of pain pattern: Early in the course of CP, the pain may occur in recurrent attacks; as the condition progresses, the pain tends to become more continuous
Abdominal Pain • Pain is reported to improve or resolve with time in the majority of patients with CP • Mullhaupt et al reported that 240 of 251 patients (95.6%) with alcoholic pancreatitis achieved pain relief after a median time of 10 years (range, 0–30 y) and that, in the majority of patients, this pain relief coincided with the onset of exocrine and endocrine pancreatic insufficiency (pancreatic “burnout”). • Abstainers have a slower rate of deterioration of pancreatic function and a better response to pain therapy than patients with non abstinence • Mullhaupt et al. Impact of etiology on the painful early stage of chronic pancreatitis: a long-term prospective study, Z Gastroenterol43 (2005), pp. 1293–1301
Abdominal Pain • An acute attack of pancreatitis • Pancreatic pseudocyst • Portal or splenic vein thrombosis • Bile duct obstruction (associated with jaundice) • Gastric or duodenal ulcers
Pathogenesis of Pain in CP • Poorly understood and several theories have been proposed to explain pain in chronic pancreatitis • Pancreatic ductal hypertension • Peripheral Nerve Damage • Central sensitization and hyperalgesia • Oxidative stress
Complications of Chronic Pancreatitis • Pseudocyst • Bile duct or duodenal obstruction • Splenic vein thrombosis (gastric varices & GIB) • Pseudoaneurysms • Pancreatic cancer • Pancreatic fistulas (treated with octreotide) • Fat soluble deficiencies (KADE)- B12 defic 40% • Pancreatic ascites (amylase > 1000)