Download
1 / 25
250 likes | 413 Views
Page 5.31. Chapter 5 Astigmatic Image Formation. Clinical Classification of Regular Astigmatism . Fig. 5.24 Page 5.45. Example 5.11 – Correcting Astigmatism. Example 5.11. Fig 5.24 Page 5.45. Fig 5.24 Page 5.45. Example 5.11 – Correcting Astigmatism. 5. 3. 180 meridian :

E N D
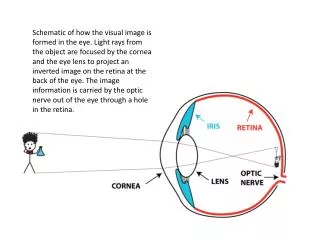
Page 5.31 Chapter 5 Astigmatic Image Formation
Clinical Classification of Regular Astigmatism Fig. 5.24 Page 5.45
Example 5.11 Fig 5.24 Page 5.45
Fig 5.24 Page 5.45 Example 5.11 – Correcting Astigmatism 5 3 180 meridian: A = Femm Fe = +60 63 = 3 D myopia (refractive). 90 meridian: A = Femm Fe = +60 65 = 5 D myopia (refractive).
3 DS Fig 6.29 Page 6.45 Fig 5.24 Page 5.45 Example 5.11 Add 3 DS in front of eye. What does the patient then see on the VA chart?
5 DS Fig 6.29 Page 6.45 Fig 5.24 Page 5.45 Example 5.11 Add 5 DS in front of eye. What does the patient then see on the VA chart?
5 DS 3 DS cyl + cyl Accom? One of the two appearances below is the valid starting point for an all focal-line based astigmatic subjective refraction. Which one?
Retina Clinical Aspects of Astigmatism Page 5.47 • In real-world vision, looking at complex objects, the uncorrected astigmat will not always be focusing focal lines or COLCs on the retina • All other parts of the interval of Sturm are elliptical in cross-section • A feature of uncorrected astigmatic vision is elliptical elongation or “distortion” (don’t confuse with the aberration, distortion) of images • This effect increases with magnitude of (uncorrected) astigmatism and with pupil diameter
Accommodation in the Uncorrected Astigmat Page 5.47 • To obtain optimum uncorrected vision, astigmats will (subconsciously) try to place the COLC on the retina • In orientation-dominant objects, the astigmat’s visual system may try to place one or other focal line on the retina – especially in city environments, where much of the landscape is horizontals and verticals • How do our five clinical types of astigmat fare when uncorrected?
Fig 5.24 Page 5.45 Page 5.47 Take the eyes that we used to define the five clinical types of astigmatism
Fig 5.24 Page 5.45 • The uncorrected CHA can accommodate to bring any part of the Interval of Sturm to the retina, IF: • Amplitude of Accommodation is sufficient • The young CHA should have reasonable vision when uncorrected • The downside is fatigue, due to constant refocusing to obtain optimum clarity Accommodation
Fig 5.24 Page 5.45 Page 5.47 Take the eyes that we used to define the five clinical types of astigmatism
Fig 5.24 Page 5.45 • The uncorrected SHA already has one focal line on the retina without accommodation • Accommodation can bring any other part of the Interval of Sturm to the retina • The demand on Amp Accom is less than for a CHA with the same magnitude of astigmatism • Fatigue is still an issue because any part of the IOS can be moved to the retina Accommodation
Fig 5.24 Page 5.45 Page 5.47 Take the eyes that we used to define the five clinical types of astigmatism
Fig 5.24 Page 5.45 • For the uncorrected MxA vision depends in part where the COLC is located (relative to the retina) in distance vision • If it is in front, vision will be worse because only the posterior FL can be moved to the retina • If it is on or behind the retina, the patient has a “choice” of COLC or posterior FL
Fig 5.24 Page 5.45 Page 5.47 Take the eyes that we used to define the five clinical types of astigmatism
Fig 5.24 Page 5.45 • With the posterior FL on the retina, the SMA obtains some clear vision at distance • Accommodation is no help because it moves the entire IOS in front of the retina • Poor uncorrected vision rather than accommodative fatigue is the main symptom for the uncorrected myopic astigmat
Fig 5.24 Page 5.45 Page 5.47 Take the eyes that we used to define the five clinical types of astigmatism
Fig 5.24 Page 5.45 • Of all uncorrected astigmats, the CMA will have the worst distance vision, but no problem with accommodative fatigue
Vision in Astigmatism (ŵ BVS) vs. Spherical Ametropia Fig. 5.25 Page 5.48 Uncorrected spherical myope Vision in the uncorrected 2D myope is “identical” to that of the 4 D astigmat with COLC on the retina COLC size is the basis for predicting magnitude of astigmatism Move the COLC to the retina with sphere. Worse vision correlates with higher astigmatism Uncorrected astigmat with COLC on retina
Clinical Aspects of Astigmatism Page 5.49 Importance of Axis Direction • For general distance vision in city/indoor environments the wtr and atr astigmat should be better off than the oblique astigmat because much of the environment is made up of horizontals and verticals • Reading performance in the uncorrected astigmat will be better if the patient can move vertical focal lines to the retina
Fig. 5.26, page 5.50 (a) Emmetropia (b) Uncorrected astigmatism; horizontal FLs on retina (b) Uncorrected astigmatism; vertical FLs on retina
L = 2 to 4 D L = 2 to 4 D Who will have an easier time reading (near vision): a 2 D wtr CMA or 2 D atr CHA, if for distance vision both have the COLC 3 D from the retina? 2 D wtr CMA 2 D atr CHA
Who will have an easier time reading distant street signs: a young 2 D wtr CHA or 2 D atr CHA, if for distance vision both have the COLC 3 D behind the retina? 2 D wtr CHA 2 D atr CHA