Download
1 / 51
600 likes | 1.63k Views
HEPARIN INDUCED THROMBOCYTOPENIA (HIT). HEPARIN-INDUCED THROMBOCYTOPENIA. Causative agents. Unfractionated heparin (UFH) (beef > pork) Continuous iv infusion Cardiopulmonary bypass Low dose sq Heparin flushes Heparin-bonded catheters Low molecular weight heparin

E N D
HEPARIN-INDUCED THROMBOCYTOPENIA Causative agents • Unfractionated heparin (UFH) (beef > pork) • Continuous iv infusion • Cardiopulmonary bypass • Low dose sq • Heparin flushes • Heparin-bonded catheters • Low molecular weight heparin • More likely to cause HIT if pt previously exposed to UFH
HEPARIN-INDUCED THROMBOCYTOPENIA Clinical manifestations • Isolated thrombocytopenia (“Isolated HIT”) • Arterial or venous thrombosis (HITT) • DVT, PE, MI, stroke, peripheral arterial occlusion • DIC, microangiopathic hemolytic anemia • Skin necrosis (at injection sites or distant) • Venous limb gangrene (? Role of warfarin) • Sudden death • ARDS • Hemorrhagic adrenal infarction
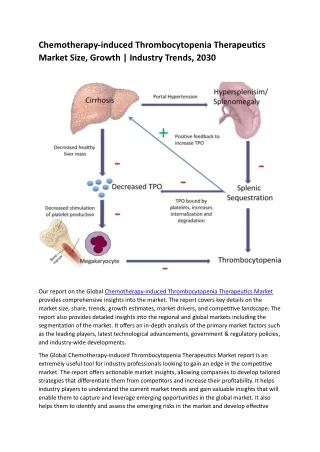
HEPARIN-INDUCED THROMBOCYTOPENIA Epidemiology • UFH > LMWH >> Fondaparinux • Duration of heparin treatment ≥ 6 days • Rarely occurs in patients < 40 years old • 2-3 fold higher incidence in women • Surgical > medical > obstetric patients • Incidence in trauma patients proportional to severity of trauma • Related to degree of platelet activation? Blood 2012; 119: 2209
HEPARIN-INDUCED THROMBOCYTOPENIA Incidence and presenting features Warkentin and Kelton, Am J Med 1996;101:502
THROMBOTIC COMPLICATIONS IN HIT Am J Med 1996;101:502
ISOLATED HIT IS ASSOCIATED WITH A HIGH RISK OF SUBSEQUENT THROMBOSIS Am J Med 1996;101:502 • Over 50% of patients presenting with “isolated HIT” had a subsequent thrombotic episode within 30 days • Substitution of warfarin for heparin after the onset of thrombocytopenia did not prevent thrombosis
UNFRACTIONATED HEPARIN IS MORE LIKELY TO CAUSE HIT THAN LMWH Randomized trial in pts having hip surgery Warkentin et al, NEJM 1995;332:1330
THE FREQUENCY OF THROMBOSIS AFTER HIP SURGERY IS MUCH HIGHER IN PATIENTS WITH HIT THAN IN THOSE WITHOUT HIT Warkentin et al, NEJM 1995;332:1330 Odds ratio for thrombosis 37 times higher in HIT pts
THE HIT INCIDENCE IN MEDICAL PATIENTS TREATED WITH LOW DOSE SQ UFH IS ABOUT 2%Girolami et al, Blood 2003;101:2955 All cases in patients receiving UFH as prophylaxis HIT associated with 40-fold increase in risk of thrombosis
LMWH IS MORE LIKELY TO CAUSE HIT IN PATIENTS WITH PRIOR UFH EXPOSUREPrandoni et al, Blood 2005;106:3049 • Prospective cohort study, 1754 medical pts • 0.8% overall incidence of HIT • 0.3% incidence if no prior UFH exposure • 1.7% incidence if prior UFH exposure • All cases in first 2 weeks • Prevalence of thromboembolism 16.6x higher in patients with HIT (29% vs 2.4%)
Development of HIT antibodies is more common in major surgery than minor surgery, and more common with UFH than LMWHResults of a prospective trial Lubenow, N. et al. Blood 2010;115:1797-1803
THROMBOSIS IN HIT MAY OCCUR WITH NORMAL PLATELET COUNT Warkentin et al, NEJM 1995;332:1330
* * * * * * * * THE PLATELET COUNT DROPS PRIOR TO THROMBOSIS IN HIT Warkentin et al, NEJM 1995;332:1330 *Thrombotic episode
Recent heparin exposure may cause “rapid onset” HIT Warkentin and Kelton, NEJM 2001;344:1286
Rapid-onset HIT is associated with re-exposure to heparin within 90 days Warkentin and Kelton, NEJM 2001;344:1286
Heparin-dependent antibodies usually disappear within 90 days an episode of HIT Warkentin et al, NEJM 1995;332:1330
DELAYED ONSET HIT Ann Intern Med 2002;136:210 • Describes 14 patients treated with heparin, discharged, and later re-hospitalized with thromboembolism and positive tests for HIT antibodies • Most patients got heparin during cardiac surgery • 12/14 had mild thrombocytopenia (66-145K) at time of thrombotic episode • Median time between discharge and readmission 14 days, maximum 40 days • 11 patients re-treated with heparin: all had clinical deterioration and worsening thrombocytopenia • 3 patients died
PF4 4 3 Antibody binds heparin-PF4 complex Fab Antibody binding to platelet FC receptor activates platelet 2 PF4 binds heparin FC 1 Activated platelet secretes PF4 Heparin HIT IS CAUSED BY ANTIBODIES AGAINST A HEPARIN-PLATELET FACTOR 4 COMPLEX FC receptor Platelet membrane
PATHOPHYSIOLOGY OF HIT Warkentin, Brit J Haematol 2003;121:535 • Heparin-PF4 complexes stimulate antibody production • Ag-Ab complex binds to and activates platelets, monocytes • Size of immune complex is critical, varies with PF4 and heparin concentrations • Inhibited by high heparin concentrations • Activated platelets release procoagulant microparticles • Activated monocytes produce tissue factor • Antibodies may cross-react with PF4 bound to endothelial cell heparan sulfate → vessel wall injury • Some HIT antibodies can activate platelets in the absence of heparin
Heparin concentration affects the size and charge of heparin:PF4 complexes and their ability to activate platelets Low heparin:PF4 ratio → small complexes 1:1 heparin:PF4 → large complexes Charge of complexes Heparin conc→ High heparin:PF4 ratio → small complexes Blood 2007;110:4253
Clinical factors may help determine the likelihood of developing HIT • Healthy volunteers given heparin or LMWH make IgM antibodies to heparin/PF4 • Pathologic HIT antibodies are usually IgG • Concomitant immune stimulus necessary to promote IgG HIT antibody formation? • Higher PF4 levels after surgery or acute illness may promote formation of larger immune complexes Blood 2007;110:4253 J Thromb Haemost 2012;10:1446
HIT Antibodies can activate platelets in the absence of heparin J Thromb Haemost 2005;3:2168
DISTINGUISHING IMMUNE FROM NON-IMMUNE HEPARIN INDUCED THROMBOCYTOPENIA • Many patients have a transient decrease in platelets within 24 hours of receiving heparin. • This is not an antibody-mediated effect and not associated with thrombosis • How can it be distinguished from HIT? • By the time course • By the clinical picture • By serology and other lab tests
Severe thrombocytopenia is rare in HIT Warkentin, Brit J Haematol 2003;121:535 • Median platelet nadir 55K • 15% had nadir >150K (diagnosed because platelet count fell more than 50% or because of clinical events) • The severity of thrombocytopenia did not predict thrombotic events
Clincal features that favor a diagnosis of HIT Blood 2012;119:2209
The 4 T score predicts a positive HIT antibody testJ Thrombos Haemost 2006;4:759
LABORATORY DIAGNOSIS OF HIT • Immunoassay for heparin-PF4 antibodies (EIA) • Very high sensitivity, rapid turnaround • “High positive” results typical of HITT • Rapid “bedside” assay • Many false positive results, not recommended • C14 Serotonin release assay (SRA) • Measures heparin-dependent platelet activation • Best predictor of thrombotic risk • Limited availability (Blood Center of SE Wisconsin), slower turnaround • A positive EIA test in a patient with a low pre-test probability of HIT according to 4T rule is likely to be a false positive
The serotonin release assay predicts thrombosis in HIT SRA and EIA negative EIA positive, SRA negative SRA and EIA positive Am J Hematol 2007;82:1037
The incidence of HIT antibody formation and risk of HIT varies among different patient populations The “Iceberg” model Warkentin, Brit J Haematol 2003;121:535
A STRONGLY POSITIVE EIA RESULT IS ASSOCIATED WITH HIGHER RISK OF SUBSEQUENT THROMBOSIS OD values in HIT vs HITT patients Thrombosis-free survival vs OD J Thrombos Haemost 2004;2:2133-7
TREATMENT OF HIT • Discontinue all heparin, including flushes • LMWH may cross-react with HIT antibodies, should not be used • If thrombosis present: give alternative thrombin inhibitor • Consider treating even if thrombosis absent (high risk of thrombosis in patients with isolated HIT) • Treatment alternatives: • Direct inhibitors • Lepirudin • Bivalirudin (little data, but approved for HIT patients having PCI) • Argatroban • Dabigatran? • Indirect inhibitors • Fondaparinux • Do not give warfarin (risk of venous gangrene)
DIRECT THROMBIN INHIBITORS • Lepirudin (Refludan®) • Recombinant form of leech anticoagulant • Clearance mainly renal (avoid in renal failure); halflife normally 80 min • Antibody formation may cause drug accumulation or anaphylaxis (rare) • Argatroban (Novastan®) • Synthetic arginine derivative • Clearance mainly hepatic (can use in renal failure); halflife 40-50 min • Both given by continuous iv infusion, monitoring aPTT • Coagulopathic patients (long baseline aPTT) difficult to monitor • No antidote for either drug
LEPIRUDIN PROPHYLAXIS IN HITBlood 2004;104:3072 • Patients: 91 patients with isolated HIT (no thrombosis) treated with lepirudin (three separate trials) • Controls: 47 contemporaneously diagnosed HIT patients without thrombosis not treated with anticoagulants
LEPIRUDIN IN HITHAT-3 trial (HIT with or without concurrent thrombosis) Cumulative incidence of death, thromboembolism or limb amputation Cumulative incidence of major bleeding J Thromb Haemost 2005; 3:2428
The risk of bleeding with lepirudin is higher with impaired renal functionHAT-3 trial data J Thromb Haemost 2005; 3:2428
LEPIRUDIN IN HITACCP RECOMMENDATIONS • Bolus 0.2 mg/kg only if life- or limb-threatening thrombosis present • Continuous infusion rate: • Cr < 1.0: 0.1 mg/kg/hr • Cr 1.0-1.6: 0.05 mg/kg/hr • Cr 1.6-4.5: 0.01 mg/kg/hr • Cr > 4.5: 0.005 mg/kg/hr • Adjust to aPTT 1.5-2.0 times baseline • Check aPTT q 4h • These doses are lower than recommended in the drug package insert
Argatroban therapy in HIT • Pooled data from 2 prospective non-randomized trials • Hazard ratio with argatroban 0.3 vs historical controls • No difference in major bleeding vs controls Chest 2006;129:1407
ARGATROBAN IN HITACCP RECOMMENDATIONS • Bolus: None • Continuous infusion: • Normal organ function: 2 mcg/kg/mon • Liver dysfunction, post cardiac surgery, anasarca: 0.5-1.2 mcg/kg/mon • Adjust aPTT to 1.5-3.0 x baseline • Check aPTT q 4h • Argatroban prolongs PT/INR, making transition to warfarin tricky
FONDAPARINUX (Arixtra®) • Synthetic polysaccharide, inhibits factor Xa preferentially • Does not typically cross-react with HIT antibodies • Long half-life (17-20 h), no antidote • SQ administration • Monitoring unnecessary • Not FDA-approved for HIT treatment • Rare reports of fondaparinux-associated HIT (NEJM 2007; 356:2653)
Fondaparinux appears to be effective and safe in patients with HIT Warkentin, Hematol Oncol Clin N Am 2010; 24:755
FONDAPARINUX DOSING • Weight based: < 50 kg: 5 mg sc daily 50-100 kg: 7.5 mg sc daily > 100 kg: 10 mg sc daily • Prophylactic dose: 2.5 mg sc daily • With renal insufficiency: CrCl 30-50 ml/min: use caution CrCl < 30: do not use
VENOUS GANGRENE Arch Intern Med 2004;164:66
Ann Intern Med 1997;127:804-12 Retrospective review of 158 cases of HIT 8/8 patients with venous limb gangrene treated with warfarin, vs 3/10 with arterial thrombosis (p=.004) Median INR 5.8 in patients with venous gangrene vs 3.1 in those who did not (p<.001) Elevated ratio of thrombin-antithrombin complex to protein C activity in patients with venous gangrene vs controls Conclusion: warfarin treatment of DVT associated with HIT may cause venous limb gangrene, possibly because of acquired defect in protein C pathway Do not start warfarin treatment until HIT resolves (platelet count returns to normal) WARFARIN MAY PROMOTE VENOUS GANGRENE IN HIT
How long should anticoagulation continue after diagnosis of HIT? • HIT with thrombosis: 3-6 months • Isolated HIT (no thrombosis): at least until platelets normal, consider continuing for 30 days
Can patients with a history of HIT be given heparin again? • Heparin should not be given while tests for heparin antibodies remain positive • If cardiac surgery cannot be delayed, use alternative anticoagulant (e.g., bivalirudin) • HIT recurrence or secondary antibody response uncommon in patients with “remote HIT” and negative HIT antibody test • Heparin administration should be limited to the intraoperative period
SUMMARY-1 • HIT typically occurs after 5+ days of exposure to unfractionated heparin • Suspect HIT if platelet count falls by > 50% during heparin administration, or if new thrombotic event occurs within 2-3 weeks of heparin exposure • Onset may be earlier if there was prior exposure to heparin within past 100 days • Onset may follow discontinuation of heparin • LMWH rarely causes HIT but may perpetuate it • Risk of thrombosis in HIT is high even if patient does not have thrombosis at time of diagnosis