Download
1 / 36
380 likes | 602 Views
Basic management of tracheostomy emergencies. Dr Harry Chan & Jackie Hylton October 30 th 2012. Tracheostomy care in perspective. 5000 tracheostomies performed / yr. 600 incidents reported to NPSA. ~ 70% incidents patients came to harm. Contents of talk.

E N D
Basic management of tracheostomy emergencies Dr Harry Chan & Jackie Hylton October 30th 2012
Tracheostomy care in perspective 5000 tracheostomies performed / yr 600 incidents reported to NPSA ~ 70% incidents patients came to harm
Contents of talk • Recognition of a tracheostomy problem 2) Basic approach to managing the tracheostomy emergency
What are the commonest tracheostomy emergencies? Blockage and obstruction Accidental displacement
How do you recognise a tracheostomy problem? General colour, distress, effort Obstruction ‘see-saw’ respiration Displacement tube appears out surgical emphysema noisy breathing from mouth vocalisation when cuff up
O2, help, assess patency oxygenation
You are asked urgently to see a patient who has been stepped down from the High Dependency Unit yesterday. You are told that he is not a laryngectomy patient He appears breathless, sweaty and has an obstructed breathing pattern……… What would you do?
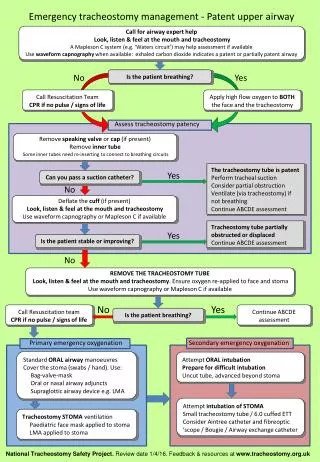
7 steps • Oxygen • Help • Look, listen and feel • Remove possible obstructing parts • Insert suction catheter • Deflate tracheostomy cuff • Remove tracheostomy tube
OXYGEN 1 To the tracheostomy…………….
And to the face……..if there is a possible patent upper airway
HELP 2 ENT ICU Anaesthesia
In the ideal world…………….. A Water’s circuit A capnograph trace
REMOVE ANY OBSTRUCTING PARTS 4 Speaking valves Humidification devices Any inner cannula
5 INSERT A SUCTION CATHETER
The patient is still deteriorating and becomes more hypoxic What now?
6 DEFLATE THE TRACHEOSTOMY CUFF If present, deflate cuff
The patient still deteriorates and is severely hypoxic now What next?
7 steps • Oxygen • Help • Look, listen and feel • Remove possible obstructing parts • Insert suction catheter • Deflate tracheostomy cuff • Remove tracheostomy tube
The patient stops breathing What are your options for oxygenating and ventilating the patient now?
Basic emergency oxygenation Cover stoma with a swab
Airway expert emergency oxygenation options Oral intubation Railroading an Aintree catheter over a fibreoptic scope
You arrive at a cardiac arrest on the ward to a patient who has had a laryngectomy in the past….. He is not breathing What would you do now?
Pre - laryngectomy Post - laryngectomy
The laryngectomy patient • In many ways, more straight forward – there is only one potential airway… You cannot bag mask ventilate or intubate via the normal oral route You can still go through the 7 steps, just avoid the upper airway!
Summary Tracheostomy emergencies usually relate to obstruction or displacement of tubes Initial management includes 1)O2 2)help 3) assessment of breathing 4) removing possible obstructions 5) using a suction catheter to test patency 6) Deflating any cuff 7) Removing the tracheostomy tube if required Management of the laryngectomy patient is limited to the neck