Download
1 / 29
290 likes | 437 Views
Chief’s Morning Report. July 11, 2011. Disclaimer: There are graphic pictures to keep the attention of the audience. HPI.

E N D
Chief’s Morning Report July 11, 2011
Disclaimer: There are graphic pictures to keep the attention of the audience.
HPI • 43 yo male with h/o DM, Schizophrenia brought in after family called police due to patient not caring for foot ulcer. Ulcer had been present 6 months after trauma. Pt and his brother had been self caring for wound at home. Pt denied fevers, chills, drainage, pain.
PMH: as above • PSH: L calf I&D • FH: DM (mother) • Social: lives with mother (bedbound), brothers; no TED • Meds: none for 5 years • Allergies: NKDA
Physical Exam Vitals: AF, HR 100, BP 156/96, SaO2 96%, 18 General: alert, oriented, NAD HEENT: PERRLA, EOMI CV: regular rhythm, normal rate, no murmurs Pulm: BCTA, no wheezing or crackles Abdomen: soft, NTND, + BS Extremities: BLE decreased sensation to light touch, vibration, pain; L foot with erythema, edema over 5th digit with small 1cm wound over plantar aspect probed to bone; 1+ pulses
Questions: • What puts this patient at risk for infection and complications? • How can you tell if his foot is infected? • If this is infected, what organisms are you concerned about? • What should you do/order next in the management of this patient?
Guidelines for the Diagnosis and Treatment of Diabetic Foot Infections A diabetic foot infection is any inframalleolar infection in a diabetic patient including paronychia, cellulitis, myositis, abscess, necrotizing fascitis, septic arthritis, tendonitis and osteomyelitis.
What puts this patient at risk for infection and complications?
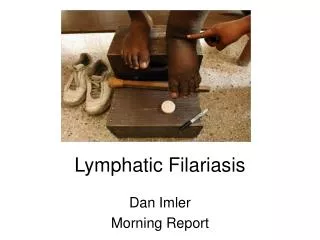
Neuropathic Ulceration Teelucksingh S, Naraynsingh V. N Engl J Med 2010;362:e26.
If his foot is infected, what organisms are you concerned about?
What should you do/order next? • CBC 9.1>9.6/28.9<508 • CRP 14.9, ESR 60 • HbA1C 10.5 • Plain films • Blood cultures: negative • Wound cultures: not done
Three views of the foot demonstrate severe osteolysis/destruction of the fifth metatarsal head and fifth digit P1 segment with osseous fragmentation noted in the region. Findings are complatible with osteomyelitis and septic arthritis. Severe surrounding soft tissue swelling is noted. No definitive soft tissue gas is seen. There is periosteal reaction along the lateral margin of the fifth metatarsal proximal diaphysis also concerning for early osteomyelitis. Loss of the cortex along with plantar aspect of the fourth metatarsal head is also concerning for osteomyelitis. Cortical thickening along the lateral margin of the fourth metatarsal diaphysis may be reactive.
Follow-up • Daily for inpatients • Initially every 2-5 days for outpatients
Prevention • A patient that has had one infection is more likely to have another. • Detection of neuropathy before complications • Educate on importance of glycemic control, appropriate footwear, avoidance of trauma and daily foot examinations. • Reinforce these measures at appointments with questioning and regular examinations.
References • Lipsky,Berendt, Deery, Embil, Joseph, Karchmer,LeFrock,Lew, Mader, Norden, Tan. Diagnosis and Treatment of Diabetic Foot Infections. Clinical Infectious Diseases 2004; 39:885–910. • Pinzur MS, Slovenkai MP, Trepman E, Shields NN. Guidelines for diabetic foot care: recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int. 2005 Jan;26(1):113-9.