Download
1 / 36
360 likes | 591 Views
Session #E6b October 6 , 2012. Disseminating CER-based Models in Primary Care for Depression and Substance Misuse through Multi-state Partnerships, Regional Implementation, and Community Engagement. Mark D. Valenti, Project Manager, Pittsburgh Regional Health Initiative

E N D
Session #E6b October 6, 2012 Disseminating CER-based Models in Primary Care for Depression and Substance Misuse through Multi-state Partnerships, Regional Implementation, and Community Engagement Mark D. Valenti, Project Manager, Pittsburgh Regional Health Initiative Robert C. Ferguson, Program Manager, Jewish Healthcare Foundation Collaborative Family Healthcare Association 14th Annual Conference October 4-6, 2012 Austin, Texas U.S.A.
Faculty Disclosure We have not had any relevant financial relationships during the past 12 months. This project is supported by grant number R18HS019943 from AHRQ. The content is solely the responsibility of the authors and does not represent the official views of AHRQ.
Objectives • Discuss how to efficiently support primary care offices to implement evidence-based care delivery models that require organizational and implementation issues to be overcome • Describe workflows and processes of the integrated care models • Explain examples of how to involve consumers in the implementation process • Describe examples of how health plans can support integrated care models
Jewish Healthcare Foundation:“A Think, Do, Train and Give Tank” • A public charity with two operating arms • Pittsburgh Regional Health Initiative (PRHI) • Health Careers Futures (HCF)
Who Are We? • Pittsburgh Regional Health Initiative (PRHI) • A not-for-profit, regional, multi-stakeholder coalition formed in 1997 • Started as an initiative of a business group, the Allegheny Conference on Community Development • PRHI’s message • Dramatic quality improvement (approaching zero deficiencies) is the best cost-containment strategy for health care
Partners in Integrated Care (PIC) – Spreading through Collaboration PRHI and the PIC Consortium were awarded a grant from the Agency for Healthcare Research and Quality (AHRQ) to disseminate and implement IMPACT+SBIRT in primary care from 9/30/10 to 9/29/13. Screening , Brief Intervention, and Referral to Treatment (SBIRT) – SAMHSA Improving Mood—Promoting Access to Collaborative Treatment (IMPACT) – University of Washington
PIC’s Deliverables under AHRQ-funded Grant • Oct. 2010 to Sept. 2011: Develop a streamlined method for implementing IMPACT+SBIRT • Oct. 2011 to Sept. 2012: Test dissemination protocol in 50-90 practices in PA, WI, and MN • Oct. 2012 to Sept. 2013: Successfully export methodology to MA and disseminate via NRHI • By Grant’s End: Position all sites for self-sustaining payment reform
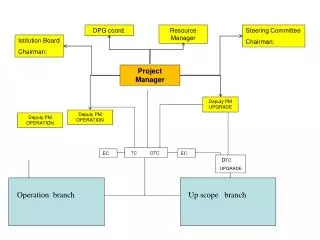
PIC - Organizational Structure State Implementation Team State Implementation Team State Implementation Team directed by Mark Valenti Dissemination to RHICs in NRHI network Principal Investigator (PI); Project Manager (PA); Work Group (WG); Health Information Technology (HIT); National Implementation and Dissemination (Nat. Imp. & Diss.); Regional health improvement collaboratives (RHIC)
PIC Model Core Components in Primary Care • Screening for depression, and alcohol and other drug misuse • Dedicated role for patient engagement, behavioral interventions, monitoring, and facilitation of team-based collaboration • Weekly caseload reviews with a consulting psychiatrist • Systematic follow-up and patient tracking • Stepped care approach to modify depression treatment
PIC Training and Coaching Didactic Role Play/Exercises Simulated Pts.
PIC Clinical Work Flow Front Desk Triage Room Exam Room Follow-Up Visits (primary care office and phone) Care manager reviews caseload with consulting psychiatrist PCP and care manager est. depression and substance-related risk/disorder Care team administers brief screens and then the PHQ-9, AUDIT, and/or DAST-10 Pt. meets eligibility for depression and substance use screening Care manager provides follow-up & monitoring PCP modifies treatment based on care team recommendations and guidelines Care manager provides brief intervention & engages patient Care manager and patient complete maintenance plan & 6 and 12 mos. follow-up
PIC Clinical Work Flow:Implemented Model 1 Front Desk Exam Room Follow-Up Visits (primary care office and phone) Care manager reviews caseload with consulting psychiatrist Care manager verbally admin PHQ-9, AUDIT, and/or DAST-10 provides brief intervention & engages patient Clinical care team administers brief screens Pt. meets eligibility for depression and substance use screening PCP est. depression & substance-related risk/disorder Care manager provides follow-up & monitoring PCP modifies treatment based on care team recommendations and guidelines One provider in an office of 10+ providers Care manager and patient complete maintenance plan & 6 and 12 mos. follow-up
PIC Clinical Work Flow:Implemented Model 2 Front Desk Exam Room CM Office Follow-Up Visits (primary care office and phone) Pt. meets eligibility for depression and substance use screening Care manager reviews caseload with consulting psychiatrist Care manager (CM) provides brief intervention & engages patient PCP scores the full screens and est. depression & substance-related risk/disorder Clinical care team administers PHQ-9, AUDIT, and/or DAST-10 Care manager provides follow-up & monitoring PCP modifies treatment based on care team recommendations and guidelines Front desk administers brief screens Care manager and patient complete maintenance plan & 6 and 12 mos. follow-up One provider office
Engaging Patients and Consumers • WIPHL • Feedback from the primary care offices’ patients • ICSI • Patient Advisory Council • Consumer awareness and engagement campaign • PRHI • Consumer Health Coalition’s training and focus groups
Engaging Patients and Consumers —Rev. Sally Jo Snyder, Consumer Health Coalition
Consumer Health Coalition • Recognizes that people experience disparate access to resources • Dedicated to the eradication of disparities in health access and outcomes • Goal is to ensure every person has the health coverage and care they need
Consumer Health CoalitionConsumer Focus Groups • Three, 1 ½ - 2 hour sessions • Six consumers • Input on patient engagement and the PIC process • Feedback on PIC materials
Findings from Consumer Focus Groups • “When I go to the doctor, I fill out the forms, but nobody talks about it.” • “The first few interactions are critical; asking intrusive questions could shut me off.” • “Where does the information go?”
Findings from Consumer Focus Groups • “The dynamic of the relationship was interesting; it was like a dance.” Suggestion to call the new role: “Your Health Supporter.”
Preliminary Findings: Recruitment • The time is ripe for implementing integrated care models (PCMHs, ACOs, etc.) • Finding a consulting psychiatrist and the reimbursement equation can present challenges • However, strong leadership and an understanding of the WIIFM can trump the concerns
Preliminary Findings: Implementation • Champions are needed at the staff, administration, and physician level in order to implement PIC • Even if a primary care site is simply adding SBIRT to an existing IMPACT infrastructure, implementation and training still require substantial effort, resources, support, and leadership
Preliminary Findings: Implementation • A registry is critical for care management, case load review, and quality improvement • Proactively address the following SBIRT-specific issues: • Stigma around substance use may be higher in primary care sites located in small, tight-knit towns • Primary care staff may make assumptions that patients will not be receptive to SBIRT (which is not the case) • A best practice for SBIRT is to begin with universal screening. • Behavioral health screens must be appropriately introduced to patients, using motivational interviewing, and incorporated into existing forms
Engaging Other Local Stakeholders • PRHI • Stakeholders Group • MCO Medicaid Medical Directors • Health Funders Collaborative Medicaid and State DHS Commercial Payers Employers Health Funders Patients and Providers • ICSI • Steering Group • Department of Human Services • MN Community Measurement • WIPHL • Advisory • Regional “Perfect Storm Campaign” • Employers
Current State of Billing for Integrated Care in Most Regions Only certain provider types can bill for services (varies by practice type and health plan) The existing codes are for specific services that do not fit the evidence-based IMPACT+SBIRT services
Breaking through FFS Limitations • DIAMOND Payment Model in Minnesota • 9 commercial health plans pay a PMPM fee • Fee covers all IMPACT services as a bundle • Certified medical groups are eligible for payment if they complete ICSI’s standardized training • Payment Model in Wisconsin • Medicaid and 13 commercial plans reimburse existing FFS codes for SBIRT services • Unlicensed professionals authorized to bill with 60 hours of training
Efforts to Create a Payment Model to Sustain PIC in Southwestern Pennsylvania Idea: As a neutral convener, PRHI could convene a collaborative meeting with all of the PH and BH MCOs in southwestern PA MEDICAID PHYSICAL HEALTH MCOs PRHI PIC PRACTICES Lesson Learned: PRHI cannot serve as a neutral convener under anti-trust laws MEDICAID BEHAVIORAL HEALTH MCOs Disclaimer: This did not occur
Efforts to Create a Payment Model to Sustain PIC in Southwestern Pennsylvania New Strategy: The State Medicaid Office could convene a meeting with all of the PH and BH MCOs in southwestern PA MEDICAID PHYSICAL HEALTH MCOs PRHI State Medicaid Office PIC PRACTICES MEDICAID BEHAVIORAL HEALTH MCOs Lesson Learned: The Office of Behavioral Health at the State- and County-level should be at the table as well
Efforts to Create a Payment Model to Sustain PIC in Southwestern Pennsylvania Strategy 3: With oversight from the State, facilitate meetings with the PH MCOs, BH MCOs, and the State and County offices of behavioral health MEDICAID PHYSICAL HEALTH MCOs PRHI State Medicaid Office PIC PRACTICES State Medicaid BH Office MEDICAID BEHAVIORAL HEALTH MCOs Lesson Learned: Precedents do not exist that include a collaborative approach between all of these parties (to be determined) County BH Office
Preliminary Findings: Dissemination • Train-the-trainer sessions must occur within the first few weeks when disseminating to multiple organizations • Common terminology is desirable but not attainable; however, operational definitions are attainable • Cultural and regional differences trump standardized terminology and training/implementation strategies. • It is important to have: • A regional entity/forum that advances the model • An entity/forum that provides training and coaching
PIC’s Anticipated Outcomes Using Required Data Fields and Measurements Specs • Depression process • 20% eligible and 50% enrolled • Substance use process • 20% eligible, 50% with brief intervention, 15% with specialty treatment entry if recommended • Depression outcomes (symptoms of depression) • 50% in response (≥50% reduction in symptoms as measured by PHQ-9) and 30% in remission (PHQ-9<5) at 6 mos. • Alcohol and drug outcomes (quantity and frequency of use) • 20% reduction in number of “binge drinking” days at 6 mos. • 30% reduction in number of drug use days at 6 mos.
Next Steps Partners in Integrated Care (AHRQ) • Continue practice facilitation and evaluation • Implement in MA around May 2013 with MHQP • Create a sustainable payment paradigm • Disseminate materials and tools through NRHI • As a Sub-awardee in the Health Care Innovation Award led by ICSI, implement a collaborative care model for depression plus diabetes and/or cardiovascular disease Care Of Mental, Physical, And Substance use Syndromes (COMPASS) (CMMI)
Questions and Answersand Discussion How could PIC be spread in your community through public policy, practice facilitation, and consumer engagement?
Session Evaluation Please complete and return theevaluation form to the classroom monitor before leaving this session. Thank you!