Download
1 / 1
10 likes | 105 Views
Randomized Phase II Trial of Extended versus Standard Neoadjvant Therapy for Esophageal Cancer NCCTG (Alliance) Trial N0849

E N D
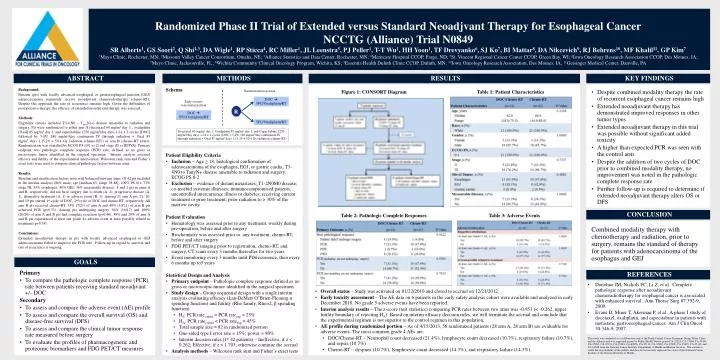
Randomized Phase II Trial of Extended versus Standard Neoadjvant Therapy for Esophageal Cancer NCCTG (Alliance) Trial N0849 SR Alberts1, GS Soori2, Q Shi1,3, DA Wigle1, RP Sticca4, RC Miller1, JL Leenstra5, PJ Peller1, T-T Wu1, HH Yoon1, TF Drevyanko6, SJ Ko7, BI Mattar8, DA Nikcevich9, RJ Behrens10, MF Khalil11, GP Kim7 1Mayo Clinic, Rochester, MN; 2Missouri Valley Cancer Consortium, Omaha, NE; 3Alliance Statistics and Data Center, Rochester, MN; 4Meritcare Hospital CCOP, Fargo, ND; 5St. Vincent Regional Cancer Center CCOP, Green Bay, WI; 6Iowa Oncology Research Association CCOP, Des Moines, IA; 7Mayo Clinic, Jacksonville, FL; 8Wichita Community Clinical Oncology Program, Wichita, KS; 9Essentia Health Duluth Clinic CCOP, Duluth, MN; 10Iowa Oncology Research Association, Des Moines, IA; 11Geisinger Medical Center, Danville, PA • ABSTRACT • METHODS • RESULTS • KEY FINDINGS Background: Patients (pts) with locally advanced esophageal or gastroesophageal junction (GEJ) adenocarcinoma commonly receive neoadjuvant chemoradiotherapy (chemo-RT). Despite this approach the rate of recurrence remains high. Given the difficulties of postoperative therapy, the efficacy of extended neoadjuvant therapy was assessed. Methods: Eligibility criteria included T3-4,N0 – Tany,N(+) disease amenable to radiation and surgery. Pts were randomized to either arm A (docetaxel 60 mg/m2 day 1 , oxaliplatin [Oxal] 85 mg/m2 day 1, and capecitabine 1250 mg/m2/day days 1-14 x 2 cycles [DOC] followed by 5-FU 180 mg/m2/day continuous IV through radiation + Oxal 85 mg/m2 days 1,15,29 + 50.4 Gy radiation (chemo-RT)) orarm B (chemo-RT alone). Randomization was stratified by ECOG PS (0/1 vs 2) and stage (II vs III/IVA). Primary endpoint was pathologic complete response (PCR) rate, defined as no gross or microscopic tumor identified in the surgical specimen. Interim analysis assessed efficacy and futility of the experimental intervention. Wilcoxon rank sum and Fisher’s exact tests were used to compare clinical/pathologic factors between arms. Results: Baseline and stratification factors were well balanced between arms. Of 42 pts included in the interim analysis (86% male; age [median 63, range 38-88], 100% PS 0/1; 71% stage III; 55% esophagus, 40% GEJ; 36% measurable disease), 4 and 1 pts in arms A and B, respectively, did not have surgery due to death (A, 2), progressive disease (A, 1), alternative treatment (A, 1) or adverse event (B, 1). Among 21 arm A pts, 21, 20, and 19 pts started 1st cycle of DOC, 2nd cycle of DOC and chemo-RT, respectively. All arm B pts received chemo-RT. 33% (7/21) of arm A and 48% (10/21) of arm B pts achieved PCR (p=0.53). Among pts undergoing surgery, 94% (16/17) and 100% (20/20) of arm A and B pts had complete resection (p=0.46). 38% and 29% of arm A and B pts experienced at least one grade 4+ adverse event at least possibly related to treatment (p=0.74). Conclusions: Extended neoadjuvant therapy in pts with locally advanced esophageal or GEJ adenocarcinoma failed to improve the PCR rate. Follow-up in regard to survival and rate of recurrence is ongoing. Schema • Despite combined modality therapy the rate of recurrent esophageal cancer remains high • Extended neoadjuvant therapy has demonstrated improved responses in other tumor types • Extended neoadjuvant therapy in this trial was possible without significant added toxicity • A higher than expected PCR was seen with the control arm • Despite the addition of two cycles of DOC prior to combined modality therapy, no improvement was noted in the pathologic complete response rate • Further follow-up is required to determine if extended neoadjuvant therapy alters OS or DFS Figure 1: CONSORT Diagram Table 1: Patient Characteristics Randomization portion DOC 5FU/Oxaliplatin/RT Early toxicity assessment portion R DOC 5FU/Oxaliplatin/RT 5FU/Oxaliplatin/RT Docetaxel 60 mg/m2 day 1, Oxaliplatin 85 mg/m2 day 1, and Capecitabine 1250 mg/m2/day days 1-14 x 2 cycles [DOC]; 5-FU 180 mg/m2/day continuous IV through radiation + Oxal 85 mg/m2 days 1,15,29 + 50.4 Gy radiation (chemo-RT) Patient Eligibility Criteria • Inclusion – Age ≥ 18, histological confirmation of adenocarcinoma of the esophagus, EGJ, or gastric cardia; T3-4N0 to TanyN+ disease amenable to radiation and surgery; ECOG PS 0-2 • Exclusion – evidence of distant metastases; T1-2N0M0 disease; co-morbid systemic illnesses; immunocompromised patients; uncontrolled intercurrence illness or diabetes; receiving current treatment or prior treatment; prior radiation to > 30% of the marrow cavity Patient Evaluation • Hematology was assessed prior to any treatment, weekly during pre-operation, before and after surgery • Biochemistry was assessed prior to any treatment, chemo-RT, before and after surgery • FDG PET/CT imaging prior to registration, chemo-RT, and surgery, CT scans every 3 months thereafter for two years • Event monitoring every 3 months until PD/recurrence, then every 6 months up to5 years Statistical Design and Analysis • Primary endpoint – Pathologic complete response defined as no gross or microscopic tumor identified in the surgical specimen. • Study design – Group sequential design with a single interim analysis evaluating efficacy (Lan-DeMets O’Brien-Fleming α spending function) and futility (Rho family, Rho=2, β spending function) • H0: PCR ratecontril = PCR rateexp = 25% • HA: PCR ratecontril < PCR rateexp = 45% • Total sample size = 82 in randomized portion • One-sided type I error rate = 15%; power = 80% • Interim decision rules (1st 42 patients) – Ineffective, if z < -0.262; Effective, if z > 1.703; otherwise continue the accrual • Analysis methods – Wilcoxon rank sum and Fisher’s exact tests • CONCLUSION Table 2: Pathologic Complete Responses Table 3: Adverse Events Combined modality therapy with chemotherapy and radiation, prior to surgery, remains the standard of therapy for patients with adenocarcinoma of the esophagus and GEJ • GOALS Primary • To compare the pathologic complete response (PCR) rate between patients receiving standard neoadjvant +/- DOC Secondary • To assess and compare the adverse event (AE) profile • To assess and compare the overall survival (OS) and disease-free survival (DFS) • To assess and compare the clinical tumor response rate measured before surgery • To evaluate the profiles of pharmacogenetic and proteomic biomarkers and FDG PET/CT measures • REFERENCES • Donohue JM, Nichols FC, Li Z, et al. Complete pathologic response after neoadjuvant chemoradiotherapy for esophageal cancer is associated with enhanced survival. Ann Thorac Surg 87:392-9, 2009. • Evans D, Miner T, Akerman P, et al. A phase I study of docetaxel, oxaliplatin, and capecitabine in patients with metastatic gastroesophageal cancer. Am J Clin Oncol 30:346-9, 2007. • Overall status – Study was activated on 01/22/2010 and closed to accrual on 12/21/2012. • Early toxicity assessment –The AE data on 6 patients in the early safety analysis cohort were available and analyzed in early December 2010. No grade 5 adverse events have been reported. • Interim analysis results – The z-score (test statistics) comparing PCR rates between two arms was -0.953 (< -0.262, upper futility boundary of rejecting HA). Based on interim efficacy decision rules, we will terminate the accrual and conclude that the experimental regimen is not superior to the control regimen in this population. • AE profile during randomized portion – As of 4/15/2013, 56 randomized patients (28 arm A, 28 arm B) are evaluable for adverse events. The most common grade 4 AEs are: • DOC/Chemo-RT – Neutrophil count decreased (21.4%), lymphocyte count decreased (10.7%), respiratory failure (10.7%), and sepsis (10.7%) • Chemo-RT – dyspnea (10.7%), lymphocyte count decreased (14.3%), and respiratory failure (14.3%). This study was conducted as a collaborative trial of the North Central Cancer Treatment Group, Mayo Clinic and the Alliance and was supported in part by Public Health Service grants CA-25224, CA-37404, CA-35431, CA-35269, CA-35101, CA-35448, CA-60276, CA-35113, CA-35267, CA-35090, CA-35415, CA-35119, and CA-63848 from the National Cancer Institute, Department of Health and Human Services. The content is solely the responsibility of the authors and does not necessarily represent the views of the National Cancer Institute or the National Institute of Health.



















