Download
1 / 36
360 likes | 450 Views
Urinalysis in CLInical diagnosis. Dr. E. I. Ugwuja PhD; MIBMS (UK) Department of Chemical Pathology, ESUT College of Medicine, Enugu, Nigeria. What is urinalysis ?. The practice of examining urine as an aid in the diagnosis and in following the course of treatment of disease.

E N D
Urinalysis in CLInical diagnosis Dr. E. I. Ugwuja PhD; MIBMS (UK) Department of Chemical Pathology, ESUT College of Medicine, Enugu, Nigeria
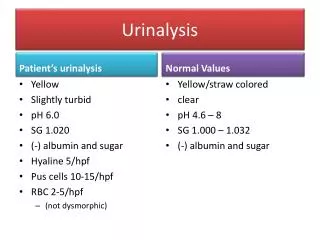
What is urinalysis ? • The practice of examining urine as an aid in the diagnosis and in following the course of treatment of disease. • Conducted as part of most medical examinations and most health examinations; may be the only examination in some cases. • Has advantage of being non-invasive, tests are sensitive for early detection of disease, methodology is convenient; minimal equipment needed
Urinalysis : window in to the patient • A complete urinalysis is a window into the patient- many different tests can be conducted and information obtained about several organs and systems simultaneously • Many common pathologic states may be recognized by urine study • Urine testing may be conducted : - In the laboratory - on the wards • In the out-patient clinics • In the admitting ward • In the physician’s office • By the patient in his home
Classification of urinalysis • Urinalysis : • Physico-chemical (Macroscopic)- appearance, colour, odour etc • Biochemical- constituents; glucose, Bilirubin, protein, UBG, bile pigments, ketone bodies etc • Microscopic examination of sediment • Urine studies supplement and complement other laboratory investigations and observations made by the physician • Urine is the most extensively studied of all body fluids.
changes in urine composition with diseases • The amount of urine passed may be decreased or possibly increased in disease (DM, DI, CRF/ARF) • The colour of urine may be changed owing to the presence of such abnormal components as blood or Bilirubin (Liver disease, haemolysis, renal disease, drugs etc) • Mucin may cause the urine to be stringy (normal / inflammation) • In certain types of disorders, the odour of the urine may be altered (PKU, MSUD, DKA) • Medical & scientific literature growing with new observations and studies describing changes in urine associated with disease.
Overview of urinalysis in clinical diagnosis • Urinalysis has been and is still invaluable in the diagnosis of: • Liver disease – bile pigments etc in urine • Classification of jaundice • Disorders of carbohydrate metabolism- Glycosuria; Non-glucose reducing sugars • Diabetes mellitus & insipidus- glucosuria/ very low SG or osmolality • Renal disease- proteinuria; haematuria • Nephrotic syndrome- massive (heavy) proteinuria • Inherited metabolic disorders (IBEM)-PKU, alkaptonuria etc • Endocrine disease- ketogenic steroids • Pregnancy- β-hCG • Toxic states- Pb toxicity (ALA; Coproporphrin), salicylates, Hg • Nutritional disorders- FIGLU,MMA • Antioxidant status- Ascorbate saturation test • Drug abuse (testing of sports men) • Malignancy- in melanoma • Starvation- ketone bodies
Urinalysis in liver disease • Analysis for bile pigments in urine is invaluable in the initial assessment of a patient with liver disease • Bilirubinuria is always pathological- once bilirubin is found in urine, it excludes pre-hepatic or haemolytic jaundice ( left with hepatic & obstructive or cholestatic). • Urinalysis helps to narrow the diagnosis in liver disease • Absence of bilirubin in urine & a raised urobilinogen level suggests prehepatic jaundice(see table 1 below)-table is only a rough guide , particularly as more than one form of jaundice can exist concurrently.
Disorders of cho metabolism/ reducing substances in urine • The Benedict’s qualitative test based on the reduction to red cuprous oxide of blue cupric sulphate in alkaline solution has been of great value in the study of disorders of carbohydrate metabolism • The detection, identification, and quantification of reducing substances in urine has long been of interest in chemical pathology and diagnostic medicine in general • Advances in techniques have greatly simplified the task. • Three questions most commonly need to be answered: • Is glycosuria present? • To what degree (severity)? • If the reducing substance detected is not glucose, what is it?- alternative investigative pathway
Reducing substances in urine cont’d • Question 1 is asked during diagnosis of or suspected DM or during tx • Question 2 is for regulation of treatment of a diabetic • Question 3- a # of other reducing substances can occur in urine: • Lactose (especially in pregnancy & lactation) • Galactose • Fructose • Pentoses (excessive intake or IBEM) • Salicyluric acid (salicylate therapy, aspirin) • Creatinine & uric acid in concentrated urine • Glucuronates from some drugs • Glutathione (GSH) • Of the reducing substances of interest glucose is the most important in pathology, and positive tests (Benedict’s or clinitest) should be checked in cases of doubt by a specific test for glucose (clinistix) • Clinitest- This tablet test is based on the same principle as Benedict’s solution; some of the chemical components generate heat.
Benedict’s/ clinitest & clinistix • Benedict’s / Clinitest: Tests are not specific for glucose but will detect any reducing substance present in sufficient quantities. Their sensitivity has been adjusted so that normal concentrations of reducing substances (e.g. Uric acid and creatinine ) do not give a positive reaction. • Clinistix strips are more sensitive than clinitest. A positive clinitest with a negative clinistix should be investigated further to identify the reducing agent present- Very important in paediatric population; an inherited metabolic disease may be present • Chromatography may be indicated- simple TLC* may be adequate- may reveal Galactosuria (reflecting Galactosaemia) * TLC- Thin layer chromatography
Dm & DI • Urine from a polyuric patient may give a high SG or osmolality- if both Benedict’s & clinistix tests are positive- DM suggested. • If the SG is very low; consistently at lower limit of ref range( normal ref range 1.003-1.030) and excessive fluid intake excluded- DI may be suggested • An inappropriately low SG may indicate tubular defect of concentrating ability as in SCD apart from DI • Common causes of greatly elevated SG: -mannitol excretion -radiographic contrast media -proteinuria
Urine specific gravity • Normal USG ~ 1.015-1.030 • Theoretical extremes are : 1.003-1.035 SG may be seen in: • Excessive water ingestion • Chronic nephritis • Steatorrhoea • DI • In chronic renal failure, USG is fixed @ 1.010. The earliest manifestation of renal damage may be the inability to produce concentrated urine (Isostenuria)
Renal disease • Presence of protein in urine is commonly associated with renal disease. Common renal disease include: • Nephrotic syndrome • Nephritic syndrome • Toxic nephropathies • Renal Tubular Diseases • Nephrosclerosis • Polycystic Kidney Disease • Severe venous congestion of kidney • pyelonephrities
OTHER causes of proteinuria • Urinalysis giving a positive protein result may suggest any of the following: • Pre-eclampsia of pregnancy • Postural proteinuria (orthostatic proteinuria) • Multiple myeloma (Bence-Jones proteinuria) • Haemorrhage • Salt depletion • Febrile illness *Bence-Jones protein is present in the absence of a serum paraprotein in about 20% of proven cases of multiple myeloma Test strips are not sensitive enough to detect BJP and other globulin- more sensitive for albumin; Bradshaw,s test or the heat test in m. Myeloma?
Nephrotic syndrome • Nephrotic syndrome(NS)- usually suggested by massive proteinuria of > 3.5 g/day • NS- by far the most common cause of decreased levels of serum immunoglobulins. IgG & IgA are decreased; IgM usually normal. Synthesis of alpha-2 macroglobulin is switched; characteristically elevated while other serum proteins fractions in electrophoresis are reduced- compensatory for albumin loss and reduced oncotic pressure • Other serum biochemical changes include: reduced total protein, reduced albumin, reduced caeruloplasmin level, hypocalcaemia, increased cholesterol, increased triglycerides etc
Inherited metabolic disorders (IBEM) • Inherited metabolic disorders or inborn errors of metabolism (IBEM) first recognized from urine appearance and smell by Sir Achibald Garrod. More common ones: • PKU (phenylalanine hydroxylase deficiency) • Alkaptonuria (Homogentisic acid oxidase deficiency) • Maple syrup urine disease(MSUD) (branched chain amino acid enzyme complex deficiency) • Galactosuria (Gal-1-PUT deficiency)
Endocrine disorders • Many endocrine disorders have been studied in the past apart from DM & DI. • Glucose is not normally detected in urine; may be found in : • Cushing’s syndrome • Hyperadrenocorticism- ketogenic steroid measurements etc • Acromegally • Phaechromocytoma • Hypertyroidism • Pancreatic disorders: • Haemochromatosis • Pancreatitis • Carcinoma of the pancreas * Drugs & lower renal threshold for glucose may give spurious glycosuria- clarify
pregnancy • Urinalysis is the oldest means of definitively diagnosing pregnancy- detection of β-hCG • Lowered threshold in this condition gives spurious glucosuria, FPG or OGTT may exclude this. • Urinalysis in pregnancy may also aid monitoring of pregnancy- may exclude or confirm pre-eclampsia; proteinuria. • May also exclude UTI- healthy pregnant state • Urinary oestriol may give information about healthy pregnancy
Toxic states • Urinalysis has been employed in the diagnosis of toxic states as follows: • Pb toxicity; ALA, UPb • Arsenic • Hg • Cd • Aspirin • Fe • Paracetamol • Drugs of abuse etc
Urinalysis in Nutritional disorders • Many nutritional disorders can be investigated by urine analysis: • Ascorbate saturation test for vitamin C def • Methyl malonic acid (MMA) for vitamin B12 deficiency(indeed considered more sensitive than some blood assays) • Formimino glutamate (FIGLU) screening test for folate deficiency • Urinary thiamine used to assess B1 deficiency • Xanthurenic acid in urine for pyridoxine (B6) deficiency
Antioxidant/ oxidative stress • Ascorbate assay / saturation measure of most important water soluble antioxidant • 8-OHdG- of the DNA derived biomarker of oxidative stress, urinary 8-oxo-7,8-dihydro-2’-deoxyguanosine (8-OHdG ,8-oxodG) is the most frequently measured. It is a marker of oxidative DNA damage and a reliable predictor of the carcinogenic risk • Despite some scientific gaps that still have to be resolved, an increase in 8-OHdG is considered a risk for cancer
drugs • Urinalysis is the main stay of many drugs & drugs of abuse: • Amphetamines-formation of a coloured-complex when amines extracted from urine are reacted with diazotized metanilic • Drug screening-barbiturates, morphine, methadone, phenothiazines • Arsenic (urine preferred to blood) • Bromides • Chlorpromazine • Heroin (diacetylmorphine) • Lecgonine & benzylecgonine- drug metabolites
malignancy • Urinalysis maybe useful: • Melanogen (Thormalen’s test) in melanoma • Bence- Jones protein in multiple myeloma & other lymphoproliferative disorders • Carcinoid syndrome- HIAA in urine • VMA/ HMMA- phaechromocytoma, neuroblastom & gangloneuroma
starvation • Ketosis • Prolonged fasting • Ketosis may also be used in the assessment of appropriate DM control • One of the metabolic observations in surgical cases is ketosis and may also be used as a rough index of progress in post operative procedures.
Wilson’s disease • Increased urinary copper • Associated parameters in other tissues: • Low Cu level in blood • Low caeruloplasmin level in blood • High Cu deposit in liver (biopsy) • Kayser- Fleischers rings around the cornea (lemon coloured rings around the cornea)
Clearance tests • Most clearance tests involve the measurement of urinary constituents. • Creatinine clearance is the most common; is a convenient measure of glomerular filtration rate (GFR), clearance values approximating to those of Inulin in both health and disease unless protein loss by the kidney is severe • Creatinine clearance= UV/P; (24 h urine collection needed) Where u= urinary creatinine concentration v= volume of urine per minute p= plasma creatinine concentration * Both urine & creatinine concentrations must be expressed in similar units e.g. Mmol/l or mg/dl
pancreatitis • Measurement of amylase in urine may help in the diagnosis of pancreatitis • An advantage of urinary amylase is that because of its low molecular mass in pancreatitis serum amylase level may be due to excretion in urine- provides a means of diagnosing the disorder when the clinical index of suspicion is high
porphyria • A clinical disorder involving porphyrin metabolism • Porphyrinuria- the presence of an elevated quantity of porphyrin in the urine is manifested in most porphyrias. Porphyriuria may also be due to other causes. • The excretion of large quantitis of porphobilinogen is pathognomonic of acute intermited porphyria. • Intermediates in the haem biosynthetic pathway-abnormality may arise from genetic basis or in toxic states e.g. Pb toxicity
microalbuminuria/myglobiuria • Measurement of this low concentration of urine may enable diagnosis of incipient renal failure e.g. DM nephropathy • Myoglobinuria- can assist in detection of crush injury or unaccustomed exercise (Myoglobin found in muscle; equivalent of Hb in blood; haptoglobin level helps its differentiation from hemoglobinuria)
Syndrome of inappropriate ant diuretic hormone (SIADH) • The normal response to a low serum osmolality is for vasopressin secretion to be inhibited , resulting in the production a dilute urine. • In SIADH the urine is inappropriately concentrated in relation to the serum, indicating continuing vasopressin secretion- ectopic secretion • In SIADH, there a continued naturesis despite the low serum sodium concentration because serum volume is maintained by water retention and there is therefore no hypovolaemicstmulus to aldosterone secretion. Hyponatraemia with natiuresis can also occur in adrenal failure and renal disorders, these must be excluded before a diagnosis of SIADH can be made.
Biochemical / clinical picture of siadh (diagnostic features) • Diagnostic features of SIADH are as follows: • Hyponatraemia • Decreased plasma osmolality (reduced plasma osmolality) • Inappropriately concentrated urine (Increased urine osmolality; USG) • Continued natriuresis [>20mmol/l] • No oedema • Normal renal function • Normal adrenal function • Clinical and biochemical response to fluid restriction
Urinalysis inc Endocrinology • 17-OHCS • 17-KGS • 17-KS (Metabolites of adrenal androgens) • Urinary estrogens (Female reproduction) • VMA • Urinary catecholamine's/metanephrines • Urinary iodine • HIAA
Urinalysis as part of the total picture • The recognition and diagnosis of disease is complex (not simple). It requires the combined skill and expertise of a number of health personnel including, of course the physician. One of the tremendously important part of the picture is that provided by urine studies. • It is pertinent to recognize that in most diseases there are changing conditions which necessitates frequent laboratory studies including urinalysis.
summary • Urinalysis holds many hidden secretes which are revealed upon careful study: • Liver disease may first be suggested by bilirubinuria. • Proteinuria and hematuria are sensitive indicators of disease • Glucosuria may be the first indicator of unsuspected DM • Certain specific mental disorders may be detected by abnormal metabolites in urine • Hemolytic disturbances become apparent with excretion of Hb & increased UBG in urine • Many IBEMs can be detected in urine • Absence of ascorbate in urine suggests nutritional deficiency • Negative results with many tests which are applied to urine have very significant implications in diagnostic medicine
appreciation Thank you for your attention!