Download
1 / 12
140 likes | 284 Views
Challenges of Health Care Financing and Pharmaceuticals in Low-Income Countries of Asia ICIUM November 15 2011. Soonman KWON, Ph.D. Professor of Health Economics and Policy School of Public Health Seoul National University, Korea. 1. Amount and Source of Financial Resources

E N D
Challenges of Health Care Financing and Pharmaceuticals in Low-Income Countries of AsiaICIUMNovember 15 2011 Soonman KWON, Ph.D. Professor of Health Economics and Policy School of Public Health Seoul National University, Korea
1. Amount and Source of Financial Resources Separate financing mechanism for medicines is not desirable: Benefit package needs to cover both medical care and pharmaceuticals -> Adequate funding level and rational allocation of funds to medicines needs to be closely monitored: - Neither under-funding, nor cost inflation due to medicines -> Not just how much but also how effectively to use resources Cultural aspects of pharmaceutical consumption in Asia: role of traditional medicine Difficult to determine the optimum amount of health expenditure -> Criteria: health expenditure and health outcomes?
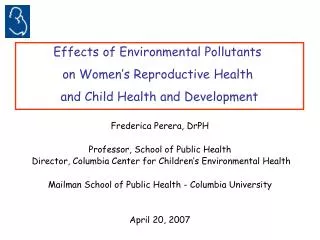
% Public Spending inTotal Pharmaceutical Expenditure Source: World Medicine Situation 2011
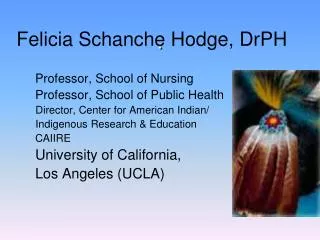
Pharmaceutical Expenditure and Health Outcomes Source: World Medicine Situation 2011
II. Financial Protection High OOP payment for health care/medicines means that health care is like a market commodity - Progressivity in OOP pay (positive Kakwani index)?: Need to examine who pays for what (e.g., Malaysia) - Access problem for the poor Catastrophic expenditure and impoverishment: >10% of HH consumption in Bangladesh, India, Nepal (WHS 2002) High OOP for Medicines in low-income countries The poor tend to rely more on drugs (than medical care) Price of medicines is high in those countries Availability of medicines in public facilities is very low -> Pharmaceutical expenditure often becomes a source of catastrophic payment for health care 5
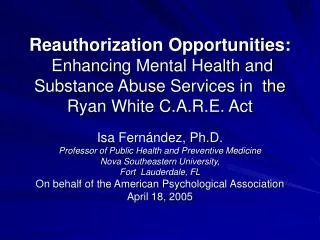
Monthly Household Expenditure on Medicines (USD PPP) Source: Calculation by Young JUNG based on World health survey 2002-2003 1) Quartiles are calculated based on household expenditure
III. Resource Generation: Tax and SHI 1. Controversy over Tax vs. SHI Comparative efficiency and equity of tax and SHI is an empirical question and contextual • Efficiency and equity in resource generation and purchasing - Question of institutional capacity: if tax administration is inequitable (e.g., income assessment), collection of SHI contribution is also likely to be inequitable - Question of purchasing to discipline public providers: purchasing can also be introduced in tax-financing Political attractiveness of ear-marking in SHI?: or MoH? Misperception that government can much reduce its role when SHI is introduced: WRONG (e.g., subsidy, price regulation, regulation of provider behavior, etc.)
2. Challenges of SHI in LI countries In low-income countries, compliance/participation is an issue in the formal sector, too (e.g., Vietnam, Philippines) <- Employer requirement to pay half of the contribution Covering the formal sector first and extending to the informal sector may not work in low-income countries - Informal sector is too big, very high cost of income assessment and premium collection - Cross subsidy by the formal sector does not work - Rapid economic development was a key factor in Japan, Korea and Taiwan (in shrinking informal sector) -> Without government subsidy, covering the informal sector through SHI is very difficult
3. Challenges of Tax-based Financing in Low-income Countries Mobilizing sufficient amount of tax revenue for health care (by increasing the policy priority to health care) may not be politically easy: Tax-financing in Asia is not as universal as Europe, targeting the poor, the better-off rely on the private sector (e.g., Sri Lanka, Malaysia) Direct tax in low-income countries can be less progressive than in high-income countries Tax financing based on local governments is likely to be geographically inequitable due to the lack of adequate equalizing (risk sharing) mechanisms: e.g., performance of decentralization? Equity of tax-based health care financing in low-income countries also depends on • Availability: delivery system in disadvantaged areas • Quality and responsiveness of the public delivery system
IV. Pooling and Coverage • Population Coverage Status of Population Coverage of SHIin Asia - 70+% (China, Mongolia), 60+% (Philippines), 40+% (Vietnam, Indonesia) - Political and financial commitment of the government: state-oriented, not by a leftist party - Political cycle in the coverage of the poor (subsidized program) With stagnant economic growth, the road to universal coverage is rugged in low-income countries Should pay more attention to the poor or need the bottom-up approach (the poor first)
2. Benefit Coverage Population coverage is not sufficient condition to (financial) risk protection, which also depends on the breadth of service coverage (types of services covered) and depth of coverage(copayment, ceiling on benefits) e.g., Philippines Potential Tradeoffs between population coverage vs. benefit coverage Controversies over cost sharing for patients • (Internal) Reference pricing: ?? Willingness of physicians to provide information on relative cost-effectiveness of alternatives ?? - Exemption for the poor and vulnerable population: admin. capacity? objective criteria? (E.g., Cambodia)
V. Purchasing and Payment Should increase the purchasing power offinancing agency - By increasing population and benefit coverage - Reducing the role of budget allocation to public providers; channeling funds (as a premium subsidy for the poor and informal sector) to purchaser/H Ins agency, which distributes funds (by reimbursement) to public and private providers, e.g., problems in Mongolia Problem of demand inducement for pharmaceuticals (by physicians): High quantity, More expensive medicines • Perverse incentive under FFS payment under non-Separation of drug prescribing (by physicians) and dispensing (by pharmacists) in Asian countries • Too low compensation for medical care or insufficient funding to hospitals (e.g., China)