Download
1 / 48
480 likes | 594 Views
Common Clinical Problems: Chest Pain . Three Questions?. What do I think this is? Is there anything else this could be? What doesn’t fit?. Chest pain: History.

E N D
Three Questions? • What do I think this is? • Is there anything else this could be? • What doesn’t fit?
Chest pain: History You are on call on the first night of your medicine rotation. Your team is called to Radiology to assess a 41 year old man who complained of chest discomfort 10 minutes ago in the CT scanner, where he was having a CT to assess the response of his metastatic colon cancer to chemotherapy.
What is the most likely diagnosis? • MI • Aortic dissection • Pericarditis • Non-CV
Prevalence in ED patients with Chest Pain • Unstable angina, MI 16-28% • Pericarditis ~2% • Aortic dissection .003% • Non-cardiovascular 72-84%
O2 • IV • Request ECG and monitor
He describes the pain as substernal, sharp, 3/10 and radiating to both shoulders. The pain is not pleuritic. There is no associated dyspnea or nausea, but he has had some sweating. His medical history is notable for Stage 4 colon cancer, metastatic to the liver and lungs, resected and being treated with chemo. He also has hypertension, hyperlipidemia, and DM2.
10 Which feature of his history would most increase the likelihood of ACS? • Pain radiating to both arms • Described as sharp • Diaphoresis
History in acute MI • Increases likelihood of AMI • Pain radiating to R arm >both arms> L arm • Syncope • Prior MI • Diaphoresis • N/V • Decreases likelihood of AMI • Pleuritic • Reproduced by palpation, sharp or stabbing, or positional
Chest pain that responds to nitroglycerin is cardiac in origin
Common sources of diagnostic error • Availability bias • The diagnosis that springs to mind: the last lecture you attended or the last patient you saw • Premature closure • Stop thinking about alternate diagnoses once a reasonable cause of symptoms is considered
Case 2 A 72 year old man with a history of diabetes, hypertension and smoking is brought to the ER with sudden, severe chest pain radiating to the back of 25 minutes duration.
Can’t miss • High mortality (aortic dissection 1% per hour) • Treatable early (with early surgery, survival ~90%) • 20%+ still missed on initial evaluation
Aortic dissection: History • Tearing or ripping chest pain (LR 10.8) • Migrating chest and back pain (LR 7.6) • Sudden onset pain • Marfan’s syndrome • Hypertension
Aortic Dissection: Exam • Any “classic” finding present in only half of all cases • Diastolic murmur (aortic insufficiency) • Unequal blood pressure in limbs (> 20 mm Hg) • Pericardial rub • Elevated JVP (tamponade) • Focal neuro deficit • Shock
Chest x-ray findings • Overall sensitivity 90% • Widened mediastinum (Sn ~ 65%) • Abnormal aortic contour (Sn ~ 70%) • Pleural effusion (Sn ~ 15%)
Consider aortic dissection: • Sudden, tearing, or ripping chest pain, especially with radiation to back • Migrating chest, back abdominal pain • Neuro deficit, pulse deficit, new AI murmur, tamponade • ECG without ST changes in patient you thought was having an MI
Case #3 An 83 year old man with a remote history of a liposarcoma of the arm presents with 4 days of fatigue, increasing dyspnea, and chest discomfort.
Temperature - C 36.6 degC Heart Rate 100 bpm High Respiratory Rate 14 br/min SBP - Noninvasive 155 mmHg High DBP - Noninvasive 83 mmHg
126 97 23 |- Ca 8.2 - - - - - - - - - |- Ca - - - ---------|-------------|------------< 111 |- Mg 2.0 ---------|-------------|------------< - - - |- Mg - - - 4.7 22 0.74 |- Phos - - - - - - - - - - - - |- Phos - - - --- 12.9 |- PT 13.7 - - - |- PT - - - 1.30 ]----------------------[ 255 |- INR 1.1 - - - ]----------------------[ - - - |- INR - - - 36 |- PTT 30 - - - |- PTT - - -
Temperature - C 37 degC Heart Rate 115 bpm High Respiratory Rate 20 br/min SBP - Noninvasive 102 mmHg DBP - Noninvasive 62 mmHg SpO2 95 % “The patient appears to be in moderate distress, ill appearing, laying in bed with an elevated rr and cool washcloth on his forehead.”
Which finding would you seek next? • Pulsus alternans • Pulsus paradoxus • Pulsus parvus et tardus
Pericardial Tamponade • Fluid increases intrapericardial pressure • With inspiration, venous return to R ventricle increases; it encroaches onto LV • Chest pain/heaviness/tightness • Symptoms & signs of poor cardiac output • Dyspnea • Elevated JVP • Tachycardia then hypotension
Pulsus paradoxus • Increased venous return with inspiration • Increased fluid in pericardial space restricts the ability of RV to stretch; excess venous return presses on ventricular septum • Decreased LV filling • Decreased blood pressure with inspiration • Also seen with severe asthma
Technique • Inflate BP cuff to above systolic BP and come down veeeerrrrry slowly • Note the pressure at which you begin to hear Korotokoff sounds during expiration • Decreased very slowly • Note the pressure at which you hear sounds in inspiration and expiration • > 10 mm Hg is abnormal
During the hospitalization he again had negative troponins, also negative HIV, and negative QuantiFERON. The pericardial fluid had 482 white cells with 77% neutrophils and 11% lymphocytes. RBC count was less than 3000. Gram stain culture, AFB, fungal were all negative from pericardial fluid.
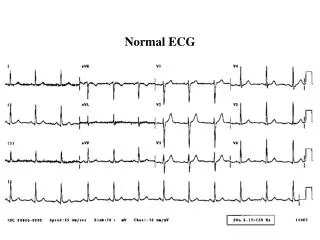
Acute Chest Pain: Next diagnostic steps • ECG • CXR • Cardiac enzymes • Further imaging as guided by history and exam: • Cardiac cath? • Echo to assess wall motion or pericarditis? • CTA or TEE or MRI to assess for dissection?
Suggestive of non-cardiac chest pain • Sharp • Pleuritic • Well circumscribed • Lasting seconds at a time • Lasting hours or days at a time • Unchanged by exertion • Associated with waterbrash (acid in mouth)
Syncope • Transient loss of consciousness, with associated loss of postural tone and spontaneous recovery. • 3% of ED visits and 1% of hospital admissions • History and exam establish diagnosis in about half • About one-third remain unexplained
Key questions in syncope • Is this really syncope? • Seizure will typically have slower return to baseline (postictal state) • Tongue biting, loss of bowel or bladder suggest seizure • Syncope can be associated with tonic clonic movmements • What’s most likely? • What can’t I miss?
Have you ever had syncope? • Yes • No • Abstain
Most common • Neurocardiogenic AKA vasodepressor AKA vasovagal syncope (25-65%) • Autonomic activation causes decreased BP, bradycardia or both • Emotion, carotid sinus pressure, situational • Medications (5-15%) • Vasodilation, bradycardia, volume depletion • Orthostatic syncope (5-10%) • Volume depletion • Autonomic insufficiency
Must not miss • Arrhythmia • Ischemia • Cardiac tamponade • Pulmonary embolism • Major acute blood loss • Valvular disease (aortic or mitral stenosis)
Key questions: • Prodrome? Suggests neurocardiogenic - sudden onset without prodrome suggests arrhythmia • Situation? Prolonged standing, physical or emotional stress, cough, micturition, etc all suggest neurocardiogenic. Syncope with exertion suggests limited cardiac output (bad). • Position? Syncope while standing suggests orthostasis, prolonged standing suggests neurocardiogenic, supine suggests arrhthmia • Any chest pain or dyspnea? • History of cardiac disease? • Family history of cardiac disease or sudden death?
Key exam • VS • Include orthostatic VS • HEENT - tongue laceration suggests seizure • Cardiac - rate and rhythm, evidence of heart failure, evidence of valvular disease • Lung - evidence of heart failure or PE • Neurologic - evidence of stroke