Download
1 / 24
360 likes | 1.68k Views
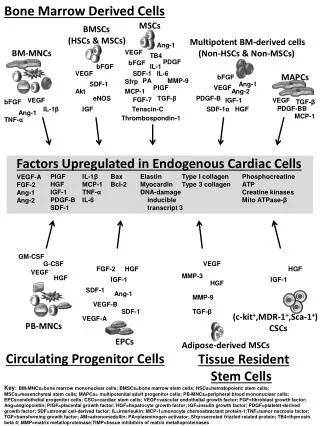
Bone marrow failure and myelodysplasia. David Lee, MD, FRCPC. Outline. Approach to pancytopenia Myelodysplasia Aplastic anemia Febrile neutropenia. Approach to pancytopenia. pancytopenia. increased destruction. sequestration. decreased production. MDS infiltration B12 def AA

E N D
Bone marrow failure and myelodysplasia David Lee, MD, FRCPC
Outline • Approach to pancytopenia • Myelodysplasia • Aplastic anemia • Febrile neutropenia
Approach to pancytopenia pancytopenia increased destruction sequestration decreased production • MDS • infiltration • B12 def • AA • drugs • viruses • radiation • immune • sepsis • hypersplenism
A practical approach pancytopenia meds spleen sepsis retics, B12/folate, ANA, SPE, abdo U/S bone marrow hypocellular hypercellular
hypercellular destruction hypersplenism MDS infiltration B12 def myelofibrosis other hypocellular aplastic anemia
Myelodysplastic syndrome (myelodysplasia or MDS) • a heterogeneous group of clonal myeloid stem cell disorders characterized by cytopenias • dysplasia of one or more cell lines is the morphologic hallmark of MDS • increased apoptosis despite increased proliferation in the marrow • a common condition in the elderly
Dysplastic erythroid maturation (dyserythropoiesis) Dyserythropoiesis Normal
MDS • cause is unknown in most patients • chemotherapy and radiation can cause MDS (ie can be a late adverse effect) • immunological and microenvironmental factors may have a pathogenic role
Clinical and laboratory manifestations • anemia • macro-, normocytic (occasionally microcytic) • oval macrocytes on blood film • neutropenia • thrombocytopenia • dysplastic features • cytogenetic abnormalities are common
Management • MDS is not known to be curable with conventional Rx such as chemotherapy • consider transplant in the young, or investigational Rx. • for most patients, treatment is supportive (RBC transfusions, treat infections) • growth factors, erythropoietin effective in some patients • lenalidomide effective in some
Prognosis of MDS • median survival: 0.3 to 12 years • worse prognosis if • increased blasts in marrow • presence of poor prognosis karyotype • 2 or 3 cytopenias • many patients with increased blasts evolve to AML
Aplastic anemia • pancytopenia with hypoplastic marrow • not due to marrow involvement with neoplastic cells • rare
Causes of aplastic anemia • drugs/chemicals • radiation • viruses: hep C, CMV, EBV, HIV • congenital (Fanconi’s anemia) • no underlying condition or external cause in 50% • immune-mediated aplasia
Relationship between radiation dosage and marrow aplasia from: Hoffman Hematology 4th ed. 2005.
Clinical and laboratory features • symptoms due to pancytopenia • no lymphadenopathy or splenomegaly • anemia is usually normocytic • hypocellular marrow is the hallmark • need to rule out other disorders
Course • survival is usually limited by the severity of neutropenia • death usually due to infection • neutrophil count < 0.2 x 109/L: median survival of less than 1 year with supportive care alone
Treatment • allogeneic stem cell transplant • immunosuppression • cyclosporine • anti-thymocyte globulin • supportive care • transfusions
The neutropenic patient • Compromise of host immunity • underlying disease • myeloma, lymphoma, acute or chronic leukemias, etc • therapy for underlying disease • chemotherapy • steroids • iatrogenic manipulations • indwelling catheters • exposure to nosocomial pathogens
Neutropenia • Neutropenia = ANC < 0.5 - 1.0 x 109/L • common adverse effect of chemotherapy • increased risk of bacterial infections increases with severity & duration of neutropenia • ~ 14% when ANC < 0.5 - 1.0 x 109/L • 24-60% risk when ANC < 0.1 x 109/L • 100% when duration of neutropenia > 5 wk • (also increasing risk of fungal infections as duration of neutropenia increases)
Febrile neutropenia • Fever > 38.3 and ANC < 0.5 - 1.0 x 109/L • At risk of sepsis! – inpatient mortality ~7% • Look for focus of infection • Must culture and start antibiotics • cover Pseudomonas aeruginosa and other gram negatives (eg. ceftazidime) • consider G-CSF (filgrastim) for current or future cycles of chemotherapy
Outline • Approach to pancytopenia • Myelodysplasia • Aplastic anemia • Febrile neutropenia