Download
1 / 1
10 likes | 102 Views
Abstract # 565. A119. Abstract. Introduction. Results. Summary. Polymorphisms in fragment C receptor ( FcγR ) are expected as a predictive biomarker of cetuximab 1-3 .

E N D
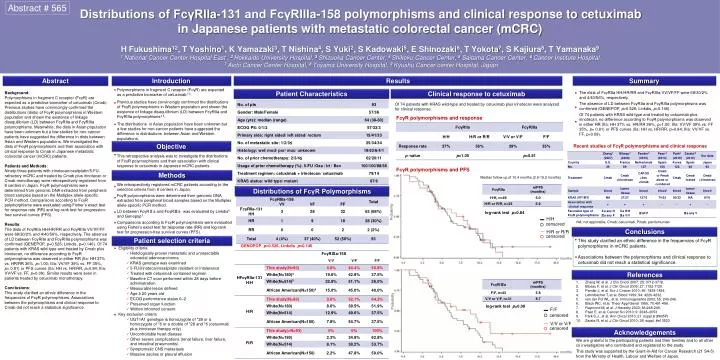
Abstract # 565 A119 Abstract Introduction Results Summary • Polymorphisms in fragment C receptor (FcγR) are expected as a predictive biomarker of cetuximab1-3. • Previous studies have convincingly confirmed the distributions of FcγR polymorphisms in Western population and shown the existence of linkage disequilibrium (LD) between FcγRIIa and FcγRIIIa polymorphisms4,5. • The distributions in Asian population have been unknown but a few studies for non-cancer patients have suggested the difference in distributions between Asian and Western populations. ● Patient Characteristics Clinical response to cetuximab The dists of FcγRIIa HH/HR/RR and FcγRIIIa VV/VF/FF were 68/30/2% and 4/40/56%, respectively. The absence of LD between FcγRIIa and FcγRIIIa polymorphisms was confirmed (GENEPOP, p=0.526; Linkdis, p=0.146). Of 74 patients with KRAS wild-type and treated by cetuximab plus irinotecan, no difference according to FcγR polymorphisms was observed in either RR (IIa: HH 37% vs. HR/RR 36%, p=1.00; IIIa: VV/VF 39% vs. FF 35%, p= 0.81) or PFS curves (IIa: HH vs. HR/RR, p=0.84; IIIa: VV/VF vs. FF, p=0.09). Background: Polymorphisms in fragment C receptor (FcγR) are expected as a predictive biomarker of cetuximab (Cmab). Previous studies have convincingly confirmed the distributions (dists) of FcγR polymorphisms in Western population and shown the existence of linkage disequilibrium (LD) between FcγRIIa and FcγRIIIa polymorphisms. Meanwhile, the dists in Asian population have been unknown but a few studies for non-cancer patients have suggested the difference in dists between Asian and Western populations. We investigated the dists of FcγR polymorphisms and their association with clinical response to Cmab in Japanese metastatic colorectal cancer (mCRC) patients. Patients and Methods: Ninety-three patients with irinotecan/oxaliplatin/5-FU-refractory mCRC and treated by Cmab plus irinotecan or Cmabmonotherapy were retrospectively registered from 8 centers in Japan. FcγR polymorphisms were determined from genomic DNA extracted from peripheral blood samples based on the Multiplex allele-specific PCR method. Comparisons according to FcγR polymorphisms were evaluated using Fisher’s exact test for response rate (RR) and log-rank test for progression-free survival curves (PFS). Results: The dists of FcγRIIa HH/HR/RR and FcγRIIIa VV/VF/FF were 68/30/2% and 4/40/56%, respectively. The absence of LD between FcγRIIa and FcγRIIIa polymorphisms was confirmed (GENEPOP, p=0.526; Linkdis, p=0.146). Of 74 patients with KRAS wild-type and treated by Cmab plus irinotecan, no difference according to FcγR polymorphisms was observed in either RR (IIa: HH 37% vs. HR/RR 36%, p=1.00; IIIa: VV/VF 39% vs. FF 35%, p= 0.81) or PFS curves (IIa: HH vs. HR/RR, p=0.84; IIIa: VV/VF vs. FF, p=0.09). Similar results were seen in patients treated by cetuximab monotherapy. Conclusions: This study clarified an ethnic difference in the frequencies of FcγR polymorphisms. Associations between the polymorphisms and clinical response to Cmab did not reach a statistical significance. ● ● Of 74 patients with KRAS wild-type and treated by cetuximab plus irinotecan were analyzed for clinical response. ● Distributions of FcγRIIa-131 and FcγRIIIa-158 polymorphisms and clinical response to cetuximab in Japanese patients with metastatic colorectal cancer (mCRC)H Fukushima12, T Yoshino1, K Yamazaki3, T Nishina4, S Yuki2, S Kadowaki5, E Shinozaki6, T Yokota7, S Kajiura8, T Yamanaka91 National Cancer Center Hospital East , 2 Hokkaido University Hospital, 3 Shizuoka Cancer Center, 4 Shikoku Cancer Center, 5Saitama Cancer Center, 6 Cancer Institute Hospital,7 Aichi Cancer Center Hospital, 8 Toyama University Hospital, 9 Kyushu Cancer center Hospital, Japan FcγR polymorphisms and response ● ● Objective Recent studies of FcγR polymorphisms and clinical response ● • This retrospective analysis was to investigate the distributions of FcγR polymorphisms and their association with clinical response to cetuximab in Japanese mCRC patients. FcγR polymorphisms and PFS Methods Median follow-up of 10.4 months (2.6-19.2 months) We retrospectively registered mCRC patients according to the selection criteria from 8 centers in Japan. FcγR polymorphisms were determined from genomic DNA extracted from peripheral blood samples based on the Multiplex allele-specific PCR method. LD between FcγRⅡa and FcγRⅢawas evaluated by Linkdis6 and Genopop7. Comparisons according to FcγR polymorphisms were evaluated using Fisher’s exact test for response rate (RR) and log-rank test for progression-free survival curves (PFS). ● Distributions of FcγR Polymorphisms ● log-rank test p=0.84 Probability ● H/H NA; not applicable, Cmab; cetuximab, Pmab; panitumumab ● censored Conclusions H/R or R/R censored Patient selection criteria • This study clarified an ethnic difference in the frequencies of FcγR • polymorphisms in mCRC patients. • Associations between the polymorphisms and clinical response to • cetuximab did not reach a statistical significance. ● GENOPOP p=0.526, Linkdisp=0.146 • Eligibility criteria • Histologically proven metastatic and unresectable colorectal adenocarcinoma • KRAS genotype was examined • 5-FU/irinotecan/oxaliplatin resistant or intolerance • Treated with cetuximab contained regimen • Baseline CT scan performed within 28 days before administration • Measurable lesion defined • Age ≥ 20 years old • ECOG performance status 0–2 • Preserved organ function • Written informed consent • Key exclusion criteria • UGT1A1 genotype is homozygote of *28 or a homozygote of *6 or a double of *28 and *6 (cetuximab plus irinotecan therapy only) • Uncontrollable heart disease • Other severe complications (renal failure, liver failure, and intestinal pneumonitis) • Symptomatic CNS metastasis • Massive ascites or pleural effusion ● ● months References • Zhang W, et al. J ClinOncol 2007; 25: 3712-3718. • Bibeau F, et al. J ClinOncol 2009; 27: 1122-1129. • Pander J, et al. Eur J Cnacer 2010; 46: 1829-1834. • Lehrnbecher T, et al. Blood 1999; 94: 4220-4232. • van derPol WL, et al. Immunogenetics 2003; 55: 240-246. • Black WC, et al. TheorAppl Genet 1985; 70:491-496. • Raymond M, et al. J Heredity 2003; 86:248-249. • Paez E, et al. Cancer Sci 2010; 9: 2048–2053 • Park S.J., et al. Ann Oncol 2010; 21: suppl.8 (#605P) • Zarata R, et al. J ClinOncol 2010; 28: suppl. #e13523 Probability log-rank test p=0.09 F/F ● censored V/V or V/F censored Acknowledgements We are grateful to the participating patients and their families and to all other co investigators who contributed and registered to the study. This study was supported by the Grant-in-Aid for Cancer Research (21 S4-5) from the Ministry of Health, Labour and Welfare of Japan. months