Download
1 / 45
3.23k likes | 13.17k Views
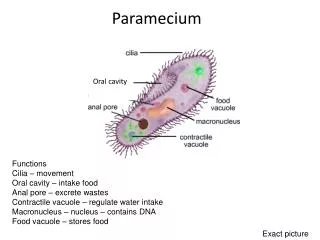
Ulcers of the oral Cavity. Dr: Arshad M.Malik Associate Professor Surgery LUMHS. ORAL CAVITY. LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES. Oral Ulcers. Definations Classifications Causes. Definition.

E N D
Ulcers of the oral Cavity Dr: Arshad M.Malik Associate Professor Surgery LUMHS
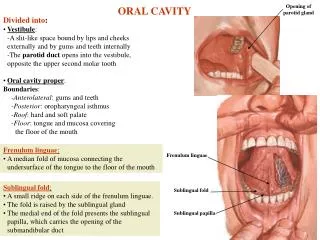
ORAL CAVITY • LIPS • TEETH • GINGIVA • ORAL MUCOUS MEMBRANES • PALATE • TONGUE • ORAL LYMPHOID TISSUES
Oral Ulcers • Definations • Classifications • Causes
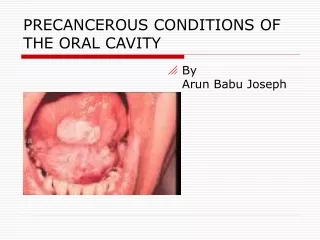
Definition • Injury to the oral mucosa may result in a localized defect of the surface in which the covering epithelium is destroyed leaving an inflammed area of exposed connective tissue. Such defects or erosions are called Ulcers.
Classification • Traumatic • Recurrent apthous stomatitis (RAS). • Ulcers associated with systemic diseases and vesicolobulous disease(Pemphigus,pemphigoid,erythema multiform) • (Dermatitis herpetiformisepidermolysisbullosa)
Causes of Oral ulceration • Infective, viral, bacterial, fungal. • Traumatic. • Mechanical • Thermal • Chemical • Factitious injury • Radiation • Eosinophilic ulcer or traumatic granuloma 3. Idiopathic • Recurrent apthous stomatitis (RAS) • Minor apthous ulcers • Major apthous ulcers • Herpitiform ulcers
Causes contd; 4. Associated with systemic diseases • Hematological diseases • Gastrointestinal diseases • Behcet syndrome • HIV infection • Other diseases 5. Associated with dermatological conditions • Lichen Plannus • Chronic discoid lupus erythromatous • Vesiculobullousdseases • Neoplastic • Squamous cell carcinoma • Other malignant tumors
Traumatic Ulcers Cheek Biting
Trauma: • Ill-Fitting dentures
Trauma: Chemical Burns
Trauma: Abrasions from Teeth
Recurrent AphthousStomatitis(RAS) • Most common ulcerative lesion of oral cavity • Recurrent, painful ulcers • Confined to soft mucosa • Subdivided into three types: • Minor aphthae • Major aphthae • Herpetiformaphthae
Apthous ulcers contd: • Etiology • A. Not understood but damaging immune response in increasingly implicated. Some of the factors are related to the cause • Immunological factors • Heredity factors • Microbiological factors • Emotional stress • Nutritional deficiencies • Allergic disorders • Hematological factors • Gastrointestinal factors.
Recurrent apthous ulcer stomatitis contd: • C/F Minor apthous ulcers • Prodromal signs appear hours before with burning and itching. • Comprise more than 80% • May be shallow and round affecting the • Non-keratinized part of the oral epithelium. • Diameter of ulcer is less than 10mm with red margin. • Heal without scarring within 7-10 days. • Tend to recur with in 1-4 months. • Site is usually the tongue, buccal mucosa, soft palate.
Recurrent apthous stomatitis Contd: • Major apthous ulcer • Larger than the minor ulcers more than 10 mm in diameter. • Site is usually similar to minor pathos ulcer. • Also involves the keratinized part of oral mucosal epithelium. • Vary in number from 1-10. • Take 4-6 weeks to heal • Heal with scarring. • Recur in less than a month time.
Recurrent apthous ulcer contd: • Herpitiform ulcers • Multiple small pin head size. Each ulcer 1-2 mm in size. • Can occur at any part of the oral cavity and as many as hundreds of small ulcers may be present. • The ulcers are present in the form of clusters or crops and some times they join to form a big ulcer. • The also heal with scarring. • Recur in less than a month time • Associated with extreme pain and discomfort.
Recurrent appthous ulcer contd: • Histopathology( Minor, Major, Herpetiform) • Mononuclear cells are found in the sub mucosa in the pre-ulcerative stage. • These mono-nuclear cells are the T4 lymphocytes and soon are outnumbered to T8 lymphocytes when ulcerative stage develops. • Macrophages and mast cells are also present in the base of ulcer.
Treatment • Major,Minor,Herpetiform ulcers. • Minor apthous ulcers require no treatment only topical gels are used to minimize the pain, as the ulcer is self limiting and heals with in 7-10 days. • Anti inflammatory gels and mouth washes are also used to prevent any further infection and to control the inflammation caused by the ulcer. • For major apthos ulcers topical steroids may be used. • In extreme severe cases systemic steroids such as prednisolone in doses 20-40 mg daily have giving promising results.
Behcet’s • Symptom complex of: • Recurrent aphthous ulcers of the mouth • Painful genital ulcers • Uveitis or conjuctivitis
Herpesvirus Infection • HSV-1 and/or HSV-2 • Primary Infection • Secondary Infection • Varicella zoster virus (HHV-3)
Herpesvirus Infection • Primary Infection • Herpetic gingivostomatitis • Younger patients • Often asymptomatic • May be associated with fever, chills, malaise • Vesicles-ulcers-crusting • Anywhere in the oral cavity
Herpesvirus Infection Primary Infection
Herpesvirus Infection • Secondary Infection • Reactivation of latent virus • Not associated with systemic symptoms • Small vesicles • Occur only on the hard palate and gingiva • Prodromal signs
Herpesvirus Infection Secondary infection
Secondary infection • Varicella zoster virus (HHV-3) • Latent infection • Oral ulcers • Dermatomal distribution
Infection • Rare • HIV/AIDS patients • Bacterial • Deep mycotic infection • Candida
Infection • Bacterial • Usually secondary infection • Primary infection: syphilis, tuberculous, or actinomycosis
Infection Bacterial-Syphilis
Infection • Mycotic • Blastomycosis • Histoplasmosis
Histoplasmosis Histoplasmosis
Infection • Candida • Candida albicans • Most common • Normal flora • Predisposing factors • White creamy patches • Nystatin oral suspension
Infection • Candida
Neoplasm • Squamous cell carcinoma (SCC) • Most common • Irregular ulcers with raised margins • May be exophytic, infiltrative or verrucoid • Mimic benign lesions grossly
Neoplasm • Squamous cell carcinoma
Dermatologic Disorders • Erythemamultiforme • Rapidly progressive • Antigen-antibody complex deposition in vessels of the dermis • Target lesions of the skin • Diffuse ulceration, crusting of lips, tongue, buccal mucosa • Self-limited, heal without scarring
Dermatologic Disorders Erythemamultiforme
Dermatologic Disorders • Lichen planus • Chronic disease of skin and mucous membranes • Destruction of basal cell layer by activated lymphocytes • Reticular: fine, lacy appearance on buccal mucosa (Wickman’sstriae) • Hypertrophic: resembles leukoplakia • Atrophic or erosive: painful
Dermatologic Disorders • Benign mucous membrane pemphigoid • Tense subepithelialbullae of skin and mucous membranes • Rupture, large erosions, heal without scarring • Sloughing (Nikolsky sign) • Bullouspemphigoid • Cutaneous lesions more common • Both show subepithelial clefting with dissolution of the basement membrane • IgG in basement membrane
Pemphigusvulgaris • Severe, potentially fatal • Jewish and Italians • Intraepithelial bullae and acantholysis • Nikolsky’s sign • Loss of intracellular bridges • Autoimmune response to desmoglein 3 • Intraepithelial clefting