Download
1 / 39
390 likes | 423 Views
Salvage Radical Prostatectomy. RJ Karnes MD, FACS Vice-Chair Associate Professor and Consultant Dept. of Urology/Urologic Oncology Mayo Clinic-Rochester. Professor Horst Zincke 1937-2011. "He was a man, take him for all in all, I shall not look upon his like again.". Radiation Recurrence?.

E N D
Salvage Radical Prostatectomy RJ Karnes MD, FACS Vice-Chair Associate Professor and Consultant Dept. of Urology/Urologic Oncology Mayo Clinic-Rochester
Professor Horst Zincke 1937-2011 "He was a man, take him for all in all,I shall not look upon his like again."
Radiation Recurrence? • Most radiation failures treated with “palliative” hormonal therapy (HT) • CAPSURE: 63% treated - recurrent or secondary treatment at mean f/u of 38 months (93% HT) • Long-term HT not without side effects • Agarwal, Cancer, 2008 • Better definition? • ASTRO: 2ng/ml >from nadir; predictive of progression not local recurrence • Nadir PSA above 1 or 1.5 ng/ml-probably worrisome?
Local Recurrence: Chance for Cure? • EORTC Bolla trial= ~20% LR only (EBRT and EBRT + ADT) • Lancet Oncology 2010 • Even at dosages to 78 Gy almost 1/3 will have a positive biopsy at 2 years • Predictive of progression compared to negative biopsy • Crook J • Late wave of metastasis from local persistence • Coen et al, Shipley, JCO 2002
My workup • Radiographic imaging: • CT scan • Bone scan • Endorectal coil MRI (3 Tesla) • Investigational:11C-choline PET/CT scan (PPV >95%)
My workup (after “OK” imaging) Standard 12 core TRUS prostate biopsy including 2 cores of SVs (seminal vesicles) • Severe treatment effect= Behave like – • Wait at least 12-24 months • Office flexible cystoscopy (anatomy, high risk disease, secondary bladder cancer) • Rare-Urodynamic study • Colonoscopy within 5 years • Stoma counseling/marking/enema bowel prep
Pattern of Spread: Importance of Seminal Vesicles • Sanctuary
Brachytherapy Failures Treated by Surgeryn=9 • All specimens whole mounted and step-sectioned • Iodine or Palladium seeds collected and counted
Benign Cancer
Rt SV Lt SV P A • Prostate map created for each specimen A Base P P A P P P P P A R L A A A = Anterior P = Posterior 33 Seeds Gleason 4+3 Tx Vol=12.5cc pT3bN0 Apex
Results Seminal Vesicle Involvement (n=6) 5 4 3 Count 2 1 0 T2aN0 T2bN0 T3aN0 T3bN0 T3bN1 T4Nx Pathologic Stage Importance of Seminal Vesicles!
Kill Zone Seed
Kill Zone Seed Cancer “Re-Growth”
“Ideal” Surgical Candidate….not unlike radiation naive • >10 year life expectancy • Coping skills • PSA < 10 ng/ml • Lower Gleason score (non 8-10) • cT1-T2 • cN- • However I do not rule out others…..
Mayo Clinic • Before 2000, Largest series n=108 (106 EBRT), `66-`96 • pT2 39%, pTxN+ 18%, R1 36% • 10 yr BCR(PSA)-free 34% • 10 yr Cancer specific survival (CSS) 70% • Amling, J Urol 1999 • Update to 2000, n=138 (127 EBRT), Median F/U 84 mths. Median age 65 yo • 10 yr CSS 77% • Ward, J Urol 2005
International Collaboration • Salvage Radical Prostatectomy (SRP)
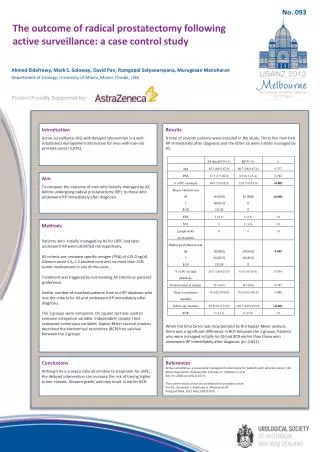
Results • Low risk subgroup: biopsy Gleason score before SRP ≤ 7 and pre-SRP PSA ≤ 4 ng/ml • 96 pts (25%) • 35 pts BCR, 4 metastases, 1 death from PCa • BCR-free probability • 62% (95% CI 49%, 72%) at 5 years • 46% (95% CI 31%, 60%) at 10 years.
Multivariable Cox proportional hazards regression to evaluate predictors of biochemical recurrence and metastases following salvage prostatectomy.
Multivariable Cox proportional hazards regression to evaluate predictors of biochemical recurrence and metastases following salvage prostatectomy.
Functional Outcomes • Urinary Incontinence • 0 ppd= 21-90% • Artificial Urinary Sphincter @ 6 mths/stabilization • Erectile Function • Pre-op EF=9-50% • Sufficient for intercourse 0-20% • Bladder neck contracture <10-20% • Rectal injury <10%
Cryo does not treat LNI and SVI Pisters, J Urol, 2009
Surgical Technique: RP+EPLND • Catheter in for 3 weeks and assess with cystogram • 5 point anastomosis (2-0 Monocryl) over 20 Fr catheter • Prepare perineum for possible Vest sutures
HIGH RISK PROSTATE CANCER SURGICAL TECHNIQUE: EXTENDED PELVIC NODE DISSECTION Spermatic Cord Common Iliac Hypogastric (Internal Iliac)
General Approach • EBRT only • Assess tissue/fat plane at bladder neck if developed then approach similar to radiation naïve, i.e. retrograde otherwise antegrade • Brachytherapy or Combined • Antegrade (take down bladder first) • Non-nerve sparing
Wide Local Excision Resection Rt NVB Beyond Prostate Apex Pararectal Fat
Wide Local Excision Rhabdosphincter Peri/Pararectal Fat
Wide Local Excision versus Bilateral Nerve Sparing Edge of pelvic fascia lateral to resected NVB Superior pedicle preserved (pelvic plexus) Superior pedicle resected to tip of SV NVB preserved
Wide Local Excision versus Bilateral Nerve Sparing Superior pedicle preserved (pelvic plexus) Superior pedicle resected to tip of SV Resected NVB NVB
Conclusions • Importance of staging (pT3b and pTxN+) • Technically challenging • Reasonable morbidity? • Survival outcomes acceptable • Diagnose earlier? • Goal-Cure; Avoid long-term hormonal therapy