Download
1 / 31
310 likes | 427 Views
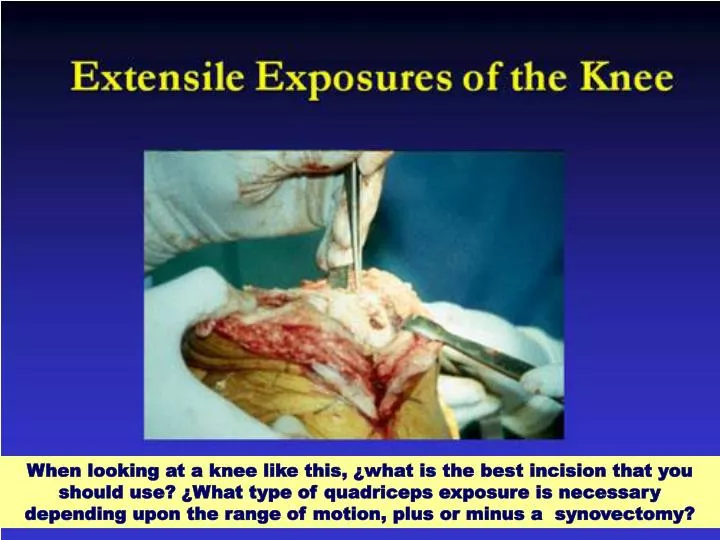
When looking at a knee like this, ¿what is the best incision that you should use? ¿What type of quadriceps exposure is necessary depending upon the range of motion, plus or minus a synovectomy? . In preoperative planning, the history, old notes, and physical exam are self-explanatory.

E N D
When looking at a knee like this, ¿what is the best incision that you should use? ¿What type of quadriceps exposure is necessary depending upon the range of motion, plus or minus a synovectomy?
In preoperative planning, the history, old notes, and physical exam are self-explanatory
Early flapping is better than late flapping. When we have a patient who we think has compromised soft tissue, we will have a plastic surgeon on hand to do a reconstructive procedure at the time of the reimplantation or the revision
Multiple incisions: We are aware of using the most lateral-based incision, because of the blood supply comes from the medial side.
If the incision is well-healed, it is 20 years old, it is mobile, it is not that deep invagination, sometimes we will choose the more medial incision, because we can do more dissection.
Consulting the infectious disease doctor is paramount if we think an infection is present
If flexion > 100 degrees and the revision is not extensive, we can try to do a midvastus or subvastus approach.
The median parapatellar is probably the most commonly used approach on both primary and revision knee arthroplasty.
A synovectomyaids in exposure. Possibly is underutilized. Getting all of the synovium out of the gutters will help lateralization of the patella and, more importantly, avoid the need for a lateral release
Slide the patellae laterally. That reduces the stresses across the patellar tendon
The purpose of these enhanced exposures is to avoid extensor mechanism disruption
You can do a beautiful knee reconstruction and if the extensor mechanism fails, then you have quite a problem.
cut it at about a 45-degree angle into the muscular-tendinous junction
Reasonable follow-up in terms of function, pain, and stiffness
Effective in the patient who has a very stiff knee. • Prior scarring of the quadriceps mechanism.
Long tibial osteotomy, 8 to 10 cm, as thick as possible Repair tibial tubercle osteotomies with cerclage wires
Arthrofibrotic knee Collateral ligaments encased in scar