Download
1 / 27
290 likes | 597 Views
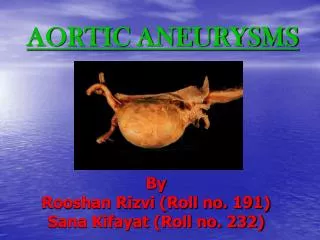
Arterial Aneurysms. Vascular Surgery Course For MRCS Military Academy, Thursday 18.08.05. Definition . Permanent localized dilatation of the affected artery over the normal diameter ~ 50% Arteriomegaly ~ 100% Aneurysms

E N D
Arterial Aneurysms Vascular Surgery Course For MRCS Military Academy, Thursday 18.08.05
Definition Permanent localized dilatation of the affected artery over the normal diameter ~ 50% Arteriomegaly ~ 100% Aneurysms As the age increases, arteries become stiffer, wider (aneurysm) and longer (tortousity)
Aetiology • Most aneurysms are caused by degenerative disease affecting the vessel (atherosclerosis) • Structural weakness & Haemodynamic forces • Damage to, and loss of intima • Reduction in the elastin and collagen content of the media • Collagen; tensile strength, adventitia • Elastin; recoil capacity, media • Risk factors • smoking, hypertension, hypercholesterolaemia
Aetiology • Laplace’s low (Tension varies directly with radius when pressure is constant) • For every increase in the radius there is a large increase in tension, leading to further enlargement of the aneurysm
Rare causes of aneurysms • Congenital • Marfan’s syndrome, Berry aneurysms • Post-stenotic • Coarctation of the aorta, Cervical rib, Popliteal artery entrapment syndrome • Traumatic • Gunshot, stab wounds, arterial punctures • Inflammatory • Takayaso’s disease, Behcet’s disease
Rare causes of aneurysms • Mycotic • Bacterial endocarditis, syphilis • Pregnancy associated • Splenic, cerebral, aortic, renal, iliac & coronary
False Due to traumatic breach in the wall The sac made up from the compressed surrounding tissue True Dilatation involving all layers of the wall Fusiform Spindle-shaped involving whole circumference Saccular Small segment of wall ballooning due to localized weakness Classification
Incidence- atherosclerotic • >90% affecting abdominal aorta • Infra-renal segment in ~95% • Male : Female ratio 4:1 • More common in western countries • 5% over 50s, 15% over 80s • Associated with iliac aneurysms in 30% • Associated with popliteal aneurysms in 10%
Anatomy of the abdominal aorta • Begins at T12, Ends at L4 • Anterior relations • Splenic vein, pancreas, duodenum • Right • Cisterna chyli, IVC, azygos vein • Left • Sympathetic trunk • Surface anatomy • Just above transpyloric plane in the mid line to a point left to the midline on the supracristal plane
branches of the abdominal aorta • Paired visceral branches • Suprarenal, renal, gonadal • Unpaired visceral branches • Coeliac, SMA, IMA • Paired abdominal wall branches • Subcostal, inferior phrenic,lumber
Clinical features of AAA • Asymptomatic in 75% • Incidentally discovered during clinical exam.or radiographic investigation • Pain • Central abdominal radiating to the back • Chronic due to stretching the vessel wall or compression/erosion of surrounding structures • Acute pain due to rupture
Clinical features of AAA • Rupture • Risk of rupture correlate with aneurysm size • Retroperitoneal, back pain, stable • Intraperitoneal, abdo/back/falnk pain, shock • 5-year rupture rate 0% in AAA <5cm • 5-year rupture rate 25% in AAA >5cm • Risk of rupture can be predicted by • High diastolic BP, COAD
Complications of AAA • Fistulation, rare • Gut, IVC, left renal vein • Thrombosis, rare • Acute lower limb ischaemia • Distal embolism • Acute ischaemia to small distal areas (trash foot) • Distal obliteration • Claudication, rest pain, gangrene
Investigation • CXR, PFT • ECG, Echo • ESR • U&Es • USS • Spiral CT with contrast • Arteriography
Management of AAA • Elective repair for AAA >6cm • Mortality 5% • Urgent repair for AAA <6cm • Developed back pain • Rate of growth >0.5cm / 6 month • Emergency repair for ruptured AAA • Mortality 50%
Elective surgical repair • 6-unit X-matched blood • Mid line or transverse incision • Aneurysm neck defined and controlled • Control of normal vessels distal to AAA • Systemic heparinization, 5000IU • AAA sac opened and thrombus removed • Back bleeding from lumber arteries controlled by sutures • Inlay tube or trouser synthetic graft • Closure of aneurysm sac over graft
Emergency surgical repair • Unstable patient, no investigation • Stable patient, USS/spiral CT • 10-unit of x-matched blood • Urinary catheter & 2 large-bore i.v. lines • Resustation to systolic BP ~100mmHg • Crash anaesthetic induction • No heparinization • Rapid entrance to abdomen & neck control • If difficult, supra-renal clamp for short period
Complications of aortic surgery • Haemorrhage, DIC • CVA • Colonic ischaemia spinal cord ischaemia • Aorto-enteric fistula • Graft thrombosis • Myocardial ischaemia • Renal failure, ARDS, MODS • False anastomotic aneurysm • Distal embolism (trash foot)
Endovascular repair of AAA • Patient unfit for surgical repair • severe cardio-pulmonary co-morbidities, hours shoe kidney, Inflammatory AAA, hostile abdo. • Anatomical suitability • Neck diameter & length • Iliac arteries diameter & tortousity • Morbidity • Endoleak, migration, kink, thrombosis • Mortality ~5% • Flow-up & durability
Inflammatory AAA • Marked fibrosis of the aneurysm wall extending to the surrounding structures • It involve the anterior and lateral aspects only • It associated with inflammatory cell infiltrate of T- , B-lymphocytes & plasma cells • The fibrosis may compress the ureters leading to renal failure • Rupture is less common and usually posterior • Pt. presents with abdo. pain, weight loss, raised ESR • Difficult surgery, therefore conservative/endovascular
popliteal aneurysms • Second most common site of atherosclerotic aneurysms • Occasionally, present with pulsatile swelling • Commonly, aneurysm thrombosis or distal emboli leading to peripheral ischaemia • USS/CT/Arteriography to confirm diagnosis • Surgical repair, resection/ligation and vein bypass • 40% of pts with PA aneurysms have an AAA
Femoral aneurysms • Can occur in isolation but usually part of generalized arteriomegaly • Often symptomless and rarely rupture • Distal emboli & thrombosis may occur • Surgical repair by using vein or synthetic graft
Splenic aneurysms • Male : female 1 : 4 • It present in child bearing period • Usually symptomless unless ruptured • Rupture rate 25% in the third trimester • Surgical treatment is indicated if the aneurysm diameter >3cm or patient is pregnant
1- AAA • A- is 4 time more common in males • B- incidence is falling in western countries • C- may safely observed if asymptomatic and >5.5cm in diameter • D- is rarely amenable to endoluminal stenting • E- is less common than popliteal aneurysms
2- AAA • A- may cause embolisation to lower limbs • B- is more common in males • C- can almost always be treated by endovascular stenting • D- can be detected by screening • E- should be operated upon when it is 5.5 cm long
3- AAA • A- typically rupture at 4cm diameter • B- extends above the renal artery in 20% of cases • C- is invariably visible on abdominal X-ray • D- is associated with coronary artery disease • E- has an association with smoking
answers • 1- A • 2- ABD • 3- DE