Download
1 / 12
190 likes | 506 Views
ECG IN HYPERKALEMIA. Potassium is most abundant intracellular cation M ost important determinant of resting membrane potential (RMP ). Mild to moderate levels of hyperkalemia Decrease TP(less negative ) Decrease RMP (less negative) Decrease RMP more than decrease TP

E N D
Potassium is most abundant intracellular cation • Most important determinant of resting membrane potential (RMP)
Mild to moderate levels of hyperkalemia • Decrease TP(less negative) • Decrease RMP (less negative) • Decrease RMP more than decrease TP • Diminish difference between two and increase excitability
Decrease in slope of upstroke of AP (dV/dT) • Major determinants of conduction velocity • Counterbalanced by decrease in RMP to TP difference • Result in ultimate increase in conduction velocity initially
Disproportional effects of varying levels of hyperkalemia on RMP and the TP • Initial increase in excitability and conduction velocity followed by their decrease as potassium level increases further
Severe hyperkalemia • Associated with increase in difference between RMP and TP • Leading to decrease in excitability • Further decrement in AP upstroke (dV/dT) overwhelms positive effect of TP decrease on conduction velocity
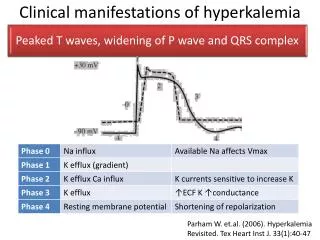
Rate of rise of phase 0 of AP (Vmax) is directly proportional to value of RMP at the onset of phase 0 • Decrease in V max levels causes a slowing of myocardial conduction manifested by progressive prolongation of P wave, PR interval and QRS complex
Mechanism for early ECG manifestations of hyperkalemia (ST depression, peaked T waves, and short-QT) • Ikris mostly responsible for K+ efflux in phases 2 and 3 • Ikrcurrents are sensitive to extracellular K+ levels • As potassium levels increase in extracellular space potassium conductance through these currents is increased • Leads to increase in slope of phases 2 and 3 • shorten repolarization time
Modulation of potassium currents byelectrolyte concentration
Effects of hyperkalemia depend on tissue involved • Atrial myocardium most sensitive • ventricular myocardium less sensitive • Specialized tissue (SA node and His bundle) least sensitive
References 1.Electrolyte disorders and arrhythmogenesis ,Nabil El-Sherif1, Gioia Turitto2, Cardiology Journal 2011, Vol. 18 2.Hyperkalemia Revisited, Walter A. Parham, MD,AliA. Mehdirad, MD, FACC ,Kurt M. Biermann, BS ,Carey S. Fredman, MD, FACC, Tex Heart Inst J 2006