Download
1 / 58
1.46k likes | 5.16k Views
Neuromuscular monitoring. Dr. S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab.DCA , Dip. Software statistics PhD ( physio ). What are we monitoring ??. Definition : Neuromuscular junction :.

E N D
Neuromuscular monitoring Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software statistics PhD (physio)
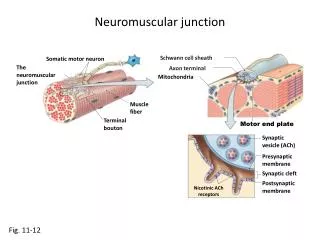
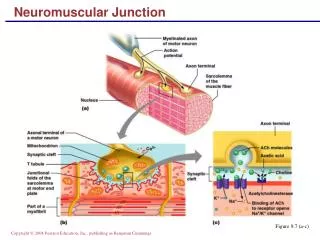
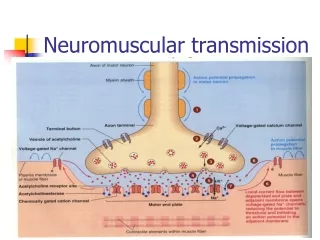
Definition : Neuromuscular junction : • the synapse between motor neuron and muscle fiber is called the neuromuscular junction
History • In 1958, Christie and Churchill-Davidson described the use of a nerve stimulator to monitor neuromuscular block. • However, it was not until the TOF pattern of stimulation was described in 1970, that such equipment came into routine clinical use.
studies • 45% of patients had residual curarization (train-of four [TOF] ratio<0.9) in the postoperative recovery room after a single intubating dose of the intermediate-acting drugs atracurium • residual curarization (TOF ratio<0.7) in 42% of patients in the postoperative recovery roomaftervecuronium
Patient is fine – let there be some residual paralysis ?? • decreased chemoreceptor sensitivity to hypoxia, • functional impairment of the pharyngeal and upper esophageal muscles, • impaired ability to maintain the airway, • increased risk for the development of post operative pulmonary complications
prolonged infusions of NM blockers • When surgery or anaesthesia is prolonged • We don’t want inadequate reversal , severe respiratory disease, morbid obesity • reversal agent may cause harm,e.g. tachy arrhythmias, cardiac failure, severe wheezing • Liver or renal dysfunction, when pharmacokinetics of muscular relaxants may be altered • Neuromuscular disorders such as myasthenia gravis or Eaton–Lambert syndrome
Reliable method • Stimulate the peripheral nerve and see the response.
Which muscle • it must have a motor element; • it must be close to the skin; • contraction in the muscle or muscle group which the nerve supplies must be visible or accessible to evoked response monitoring.
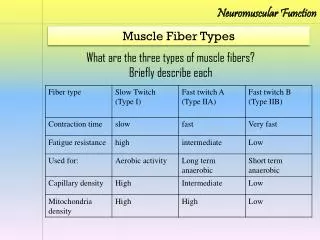
What’s the hope • Diaphragm • Larynx • 1.5 to 1.75 resistant
Stimulation • The current needed to induce depolarization in all the fibers in a nerve bundle is the maximal current. • 25 % more – supra maximal • Mono phasic, rectangular, 50 mA, 0.2 milliseconds , constant current at 0 -5 ohms • Different patterns • Battery • ECG electrodes
Stimulator - image • Subcutaneous needle electrodes • Ball electrodes described
Pattern of nerve stimulation • Single twitch stimulation. • Train-of-four stimulation. • Tetanic stimulation. • Post-tetanic count stimulation. • Double burst stimulation.
Single twitch stimulation • A single square wave supramaximal stimulus, at regular intervals, • The twitch response will only be depressed when a neuromuscular blocking agent occupies75% of the post-synaptic nicotinic receptors. • Twitch depression will need to be more than 90% in order to provide good conditions for abdominal surgery. • Onset of block – useful
Train-of-four stimulation • TOF supramaximal twitch stimuli, with a frequency of 2 Hz, • four stimuli each separated by 0.5 s. • 2 Hz for 2 seconds • Compare the first twitch to fourth
Non depolarizers and depolarizers FADE NO FADE
TOF Vs single twitch • T4 disappears at about 75% depression of T1 • T3 at 80–85% depression of T1, T2 at 90% depression. TOF count and TOF ratio
Can we correlate Extubate reverrs
Dep Vs NDPs • If larger doses of depolarizing agent are given, for example in techniques that require repeated bolus doses or infusions of succinylcholine, then a Phase 2 block may develop. • This is a block produced by a depolarizing drug which develops some of the characteristics of a non-depolarizing block. • With TOF monitoring, fade is observed.
Phase 2 block • two types • normal and abnormal cholinesterase • Can we do reversal in abnormal cholinesterase ??
DBS • allows manual (tactile) detection of subtle degree of NMB without the use of recording devices. • It involves application of two short bursts of 50Hz which are separated 750 ms,. • It consists of a series of 3 and 2 impulses (DBS 3, 2) or 3 and 3 impulses (DBS 3, 3). • D2 / D1 ratio – fade . • Fade is more easily detected manually with DBS than with TOF. • TOF – 0.4 or less , but DBS -- 0.6 detects
Tetanic stimulation • Tetanic stimulation uses a high frequency (50–200 Hz) with a supramaximal stimulus for a set time: normally 5 s. • In healthy skeletal muscle during normal movement, the response is maintained as a tetanic contraction.
Tetanic stimulation – painful • No in conscious patients • Cant be reproduced in 6-10 minutes • But • TOF can be repeated in 10 seconds
Tetanic • A frequency of 50Hz is physiological as it is similar to that generated during maximal voluntary effort. • Proponents of 100 Hz and 30 Hz are there
Fade -- why ? • large amounts of acetylcholine are released. • equilibrium between mobilization and synthesis of acetylcholine is present . • The muscle response caused by tetanic stimulation of the nerve at, for example, 50 Hz is maintained (given normal neuromuscular transmission) • acetylcholine released is many times greater than the amount necessary to evoke a response.
Fade -- why ? • When the “margin of safety” at the postsynaptic membrane (i.e., the number of free cholinergic receptors) is reduced by nondepolarizing neuromuscular blocking drugs, a typical reduction in twitch height is seen with a fade during, for instance, repetitive stimulation. • Also some presynaptic action
Fade -- also presynaptic • Pre-synaptic receptors (Bowman), implicated because: • α-Bungarotoxin, a pure post-synaptic blocker, shows no fade
Nondepolarizer Depolarizer
Post tetanic count • Can we gauge NM block if TOF is absent ?? • 50 Hz tetanic stimulation is applied for 5 s followed by 1 Hz supramaximal single stimuli after a gap of 3 s.
PTP and PTC • Tetanic stimulation facilitates the mobilization of Ach from the reserve pools to the immediate stores and increases the synthesis of Ach. • This enhanced synthesis and mobilization of Ach explains the phenomenon of posttetanicpotentiation.
use of PTC • The main use of PTC is when profound neuromuscular block is required, for example, during retinal surgery, when movement or coughing could have devastating effects.
When to use what ?? • Onset – single twitch • Intense blockade – PTC • Surgical – TOF • Recovery – TOF
Assessment of responses • Visual and tactile • Mechanomyography • Electromyography • Acceleromyography • Others
Assessment of responses to nerve stimulation (Recording devices)
Electromyography -- EMG is the recording of a compound action potential that occurs during muscular contraction, whether voluntary or evoked.