Download
1 / 57
570 likes | 574 Views
This lecture by Dr. Steven R. Lee provides an overview of addiction as a medical disease, including its definition, different use disorders, standards of care for treatment, and the interface of addiction with chronic pain.

E N D
Overview of Addiction as a Medical Disease by Steven R. Lee, MD Program Director Young Adult Addiction Program Ridgeview Institute drleemd.org
Goals of this lecture are to Understand: • The definition of Addiction • Addiction as a medical disease with descriptions of each Use Disorder • The standards of care for the treatment of addiction • The interface of the treatment of Chronic Pain with Addiction
What is Addiction? Addiction is a persistent, compulsive dependence on a substance or a behavior (i.e. gambling) even though the individual has experienced potentially harmful consequences while doing this substance or behavior.
Biological Conditioning • Once an addict has an experience that gives "pleasure" or relief, the memory of this feeling is attached to the substance or behavior that caused it. • Some individuals are genetically programed that when they take a specific substance for the first time, they have pleasure and motivation that they have never experienced before. • Some individuals feel almost total relief of their anxiety, depression, or pain that they have never had before using the substance. • They cannot stop thinking of using that substance until they use it.
Reinforcement • The repetitive use of a substance or behavior combined with the associated pleasurable feeling, imprints, into the limbic system as the best means to obtain relief and joy. • Just as practicing piano makes you a better musician, each time the addict uses that substance, the more essential it is to use it again in order to experience relief or joy.
Substance use disorder diagnosed when: There is impaired control from using a substance that clinically and functionally causes significant impairment in: -Physical health problems -Ability to perform job responsibility -Meet obligations of home, school or family -Safe judgement such as driving a car around I-285 at 100 MPH
4 Types of Addicts 1 – Those who use to get high. Usually genetically programmed to get a special high – (e.g. alcoholics and opiate addicts) 2 – Those who have co-occurring disorders or what used to be called a dual diagnosis – (e.g. alcoholic with a Generalized Anxiety Disorder) 3 – Those who do not get high but feel they have to have the substance to deal with a problem - e.g. chronic pain patient 4 – Those who can get high with multiple substances and behaviors - e.g. Alcohol, cocaine, opioids, Benadryl, gambler, sex, and more.
Neuroanatomy of Addiction Limbic System • Triage center of the brain for all sensory input to the brain • Decides what is an immediate danger and what is just information • Remembers what gives the best relief of fear or boredom • Does not remember consequences of behavior Cortex • Judgment and decision making • Memories of what is learned – good and bad • Ethical and social concerns • Restraint versus Action
Aspects of Addiction • The Obsessive-Compulsive Drive • Biological Conditioning • Unmanageability • PAWS • Craving • Use Disorders as a Medical Disease
The Obsessive-Compulsive Drive • After the first “miracle” pleasure/relief, the limbic system is constantly thinking of using the substance or doing the behavior. • Every other aspect of their life becomes secondary to the use or the "behavior" - Family, school, job, relationships, God, and the law • Repetitive use of the substance also causes a progressive increase in tolerance (decrease in response of a substance). • The addict has to use larger amounts of their substance in order to get the same benefit they got the first time. • Most addicts have fewer internal cues (i.e. less nausea with alcohol) so they can use very large amounts of substance – gross impairment
Biological Conditioning • Requires repetition of the stimulus/response behaviors – (e.g. stress as a stimulus resulting in use of alcohol with relief of stress.) • Whenever the limbic system experiences a pleasure that is quick and efficient, it never forgets. (e.g. Marijuana, alcohol, crack and meth) • What takes one second to start an addiction can take a year or longer to find behaviors that will give the limbic system the same benefits. • Teaching the limbic system to use alternative ways to get relief from boredom, anxiety, depression and fear is like teaching a dog to walk on their hind legs and for the dog to want to walk this way.
Unmanageability • Unmanageability is the inability to use a substance in moderation • After about 6 months of using a substance almost daily, most addicts begin to have unmanageability in their life because of their use. • Eventually, something significant occurs such as an auto accident, a DUI, or being fired from a job. • Unmanageability is essential for the addict to want to stop.
PAWSPost-Acute Withdrawal Syndrome • A set of persistent impairments that occur after withdrawal. • Irritability, depression, anger, anxiety, psychosis and limited to no joy. • Disturbed sleep is the most common part of PAWS. • Relapse is the most common result of PAWS if not treated. • Trazadone, Vistaril, mood stabilizers (Neurontin and Seroquel), and antidepressants should be used to treat PAWS. • The severity and longevity of PAWS depends on the potency of the drug and the length of time the drug is used. e.g. fifth of alcohol/day x 10 years = one year of PAWS
Craving • Defined as an “uncontrollable” desire. • Methamphetamine and crack cocaine addicts have some of the strongest cravings of any addiction. • Alcoholics and opiate addicts can also have severe cravings. • All opioid addicts that want recovery have to be on naltrexone/Vivitrol for a year. • Many alcoholics should be on naltrexone/Vivitrol or Campral.
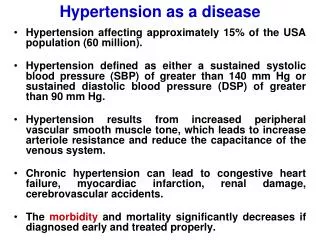
Use Disorder as a Medical Disease • Life long medical disease just like hypertension and diabetes. • Cost to treat this disease in a lifetime is the same as any other medical disease. Relapse rate is the same as that of hypertension and diabetes. • Diabetes - ~60% • Hypertension - <40% • Asthma - <40% • Addiction - ~50%
Specific Use Disorders • Nicotine • Alcohol • Marijuana • Opioids • Sedatives • Stimulants • Hallucinogens/Dissociatives
Nicotine Use Disorder #1 worst addiction in the world. • 25% of people in the US and 35% of young adults • Most loss of life – 480,000 deaths/year • Most loss of “productivity” ( as an economic measure in a society) • Most breakup of families because of premature death of a parent • Most numbers of people using an addictive substance • Hardest to treat because unmanageability not there until it is too late
Lung cancer is now the most common cancer killer of men and women. • From 2000-2010 the additional risk for women smokers jumped nearly tenfold to 25.7 x that of nonsmoking women. Men who smoke now have a 25.0x higher risk of lung cancer than nonsmokers. • COPD, Liver cancer, Type 2 diabetes, colorectal cancer, breast cancer, rheumatoid arthritis, and increase the risk of tuberculosis
Treatment Requires Wanting to Stop First, you have to really want to stop Second, prepare yourself mentally, spiritually, socially, and physically • Make a plan • Tell everyone you are going to stop • Anticipate every pitfall - including withdrawal, PAWS, and craving • Medically, cover this with either patches, Wellbutrin or Chantix • Consider psychotherapy
Alcohol Use Disorder • 15% of the United States population have an Alcohol Use Disorder. • Majority of these addicts are “closet drinkers” (no one knows that they are alcoholics). • Most have a set of genes that allow them to drink large quantities without getting sick and alcohol makes them more mentally clear, less anxious, and feel comfortable in groups of people. • Alcohol (and benzodiazepines) causes disinhibition which essentially means that it disconnects the circuits from the cortex to the limbic system such that the limbic system is in charge.
Cancer Caused by Alcohol • One in 10 of all cancers in men and one in 33 in women. • Cancers of the mouth esophagus, larynx, and pharynx increase after about one daily drink for women and two daily drinks for men. • Increase risk of colorectal cancer in men with two drinks/day. • Alcohol is a risk factor for liver cancer through cirrhosis. • Alcohol increases the risk of breast cancer. Having a glass of wine or beer on occasion is not a problem but more may cause cancer. • Approximately 6% (between 3.2% and 8.8%) of breast cancers reported in the UK each year are caused by alcohol.
Alcohol Withdrawal • Acute withdrawal takes 3 to 5 days but can last as long as 7 to 10 days if the drinker has been drinking for 20+ years. • Withdrawal can be lethal. Older age, physically debilitated, cardiovascularly compromised, also withdrawing from sedatives, amount and length of time drinking. • Detoxification has to be done inpatient because of the risk of a cardiovascular injury, seizure, and agitated delirium. • In 34 years of practice I have had 5 patients have either a stroke or a heart attack and the vital signs were normal. All were <65 and healthy.
PAWS • Immediately post detox the addict may feel extra good and be convinced that they can stay sober. This is called “being on a pink cloud”. • Quickly, nothing will feel right and sleep will be very disturbed. The alcoholic will feel the need to drink. • Aggressive medical treatment of the insomnia, the anxiety, the mood swings, and the cravings will allow the sober alcoholic a better potential to stay sober. • This is when the alcoholic needs to be around other addicts for at least the first 28 days.
Medication for PAWS • Campral calms the anxiety and irritability of the PAWS. • Neurontin can give similar benefit but Campral can also give a mild sense of wellbeing. • Naltrexone can decrease the alcoholics desire to drink but it does not work for everyone. Soon we will have a genetic test that can tell who will respond. Many African Americans do not respond. • Antabuse works only as a fear of having severe nausea and vomiting.
Cannabis Use Disorder • Marijuana heightens certain senses (appetite, sexual desire, etc.) and dulls others. • It attaches to special endocannabinoid receptors in our brain that ordinarily react to natural THC-like chemicals in the brain. • Different strains of marijuana can calm you, others stimulate you, and others can help you to go to sleep. So what is the problem with a little marijuana?
Hinders mental processes of organizing and collecting thoughts. • Difficulty thinking and problem solving • Poor short term memory • Motor skills are impaired with slow response time (driving) • Loose associations (inability to stay focused on one subject) • Altered sense of time (an hour may feel like 20 minutes or 2 hours) And if that is not enough there are other problems with some people that are more serious.
More Negative Effects • Disinhibition of some emotions at inappropriate times and places (e.g. constant laughter with your boss or with your grandmother who is sick in the hospital.) • Frustration tolerance can be poor when you are pressed to get things done though that you do not want to do. • Some have feelings of paranoia or anxiety. • Most have the “munchies” resulting in some gaining a great deal of weight • Impulsively do strange or inappropriate activities such as having sex with someone that you would never have sex with.
Addiction • ~9% of those who experiment with marijuana eventually develop a Use Disorder. • Rate of addiction goes up to 17% among those who begin use as adolescents, and 25 to 50% of those adolescents who use it daily. • Long-term use of marijuana can affect brain development when marijuana users begin using as teenagers. This is because of how the brain builds connections between the areas of the brain that are necessary for thinking, memory, and learning functions.
Opioid Use Disorder • 21.5 million Americans had a substance use disorder in 2014 • 1.9 million involving prescription pain relievers • 586,000 involved heroin. • 10% of all substance use disorders involve opioids.
Opioid Overdose • Leading cause of accidental death in the US. • Half of opioid addicts have a genetic predisposition. • These addicts have a paradoxical reaction to opioids. They become mentally clear, do not worry about problems, feel comfortable in groups, and are motivated to get boring tasks done. • Within 4 - 6 months, tolerance to these benefits decreases unless the dosage is increased. • Cost drives addicts to use heroin and eventually there is an overdose.
50% are not Genetic • Those who are 55years old and over who have chronic pain problems find that opioids give them relief. • Some do not get enough relief on smaller doses of opioids and the patient increases the dose until they overdose. • Some obtain adequate relief but other medical problems such as COPD, Anxiety Disorders, and general surgery require other meds such as benzodiazepines which increase the opioid blood levels and the patient overdoses while taking their normal dose of opioid.
Opioid Withdrawal • Withdrawal starts ~36 hours after the last opioid. • Body aches, abdominal cramping, nose running, alternating feeling very hot with sweats then very cold • Diarrhea and nausea may be severe with loss of potassium and dehydration. • Very disturbed sleep, irritability, strong craving for opioids. • This lasts 3 to 5 days but with those coming off of heavy heroin, methadone, Kratom, and Suboxone, it may last 7 or more days. • 50% of insurance companies do not cover inpatient detox.
Special Considerations • Do not detox an opioid addict unless the patient is planning to go to an addiction program because the relapse back on the opioid may kill them through an overdose. • Once they have been off of all opioids for at least 10 days, they need to be on naltrexone or Vivitrol which will block the opioid receptor and decrease craving. • Naltrexone and Vivitrol also do not allow the addict to feel the benefits of the opioid so an impulsive relapse can be quickly stopped. • The standard of care for those not able to go into a treatment program: Harm Reduction medications: Methadone or Suboxone
Chronic Pain and Opioids • Thomas Friedan, the Director of the Centers for Disease Control and Prevention has taken on Opioid Use Disorder as a major medical problem because of lethal overdoses. • In 2014 the CDC added opioid overdose prevention to its list of the top 5 public health challenges.
Opioids for Chronic pain continued This is partially based on evidence that prescriptions for opioids for chronic, noncancerous pain is: • not efficacious for pain relief • actually causes increased reported pain symptoms (Opioid-induced hyperalgesia (OHI) ) • are inherently pharmacologically addictive and disabling • that the inherent nature of opioids is that they cause depression and anxiety
My Experience • I have worked heavily with chronic pain patients for the past 20 years. • Most of my patients came from the Pain Clinic at Gwinnett Medical Center with an average age of 50 years old. • All patients had appropriate surgeries, pain procedures, spinal cord stimulators when appropriate, and still had pain. • All patients obtained at least 50% improvement on opioids and did not develop tolerance to the pain relieving qualities of the opioids. • Only the rare patient abused the opioids.
Sedative/Hypnotic Use Disorder • This addiction usually results from the use of a benzodiazepine drug either to get relief of an anxiety disorder or insomnia. • Most addicts prefer a sedative that works fast such as Xanax or Ambien. • Benzodiazepines used to treat anxiety require multiple dosing and the anti-anxiety benefits do not accumulate. • Tolerance typically develops to the anti-anxiety benefits requiring increasing the dosage then the addict is stuck on that drug at doses of 6 to 8 mg of Xanax or Klonopin per day.
Sedative Withdrawal • Similar to alcohol withdrawal except withdrawal seizures can occur 2 to 4 weeks after the last use of the benzodiazepine. • This is a potentially lethal withdrawal in terms of cardiovascular events. • Strongly recommend the use of Depakote at seizure therapeutic doses for a month to prevent withdrawal seizures • Begin treatment for the underlying anxiety disorder with an antidepressant which will take 3 to 6 weeks to start giving the patient anxiety relief.
PAWS • People who have been on a benzodiazepine for several years and have to come off of the benzo will have PAWS for as long as a year. • Anxiety, disturbed sleep, dysphoria and mood swings can been difficult to severe. • If the patient is not an addict, consider keeping the patient on the benzo if they have been on one for 10 or more years. It is almost abusive to try and stop this medication on these people.
Stimulants (Cocaine and Amphetamines) • Stimulants “squeeze out” dopamine many times greater than that which is released normally. • This release of large amounts of dopamine gives a sense of wellbeing and motivation. • When the dopamine is “spent”, the person is emotionally flat and feels exhausted until the dopamine has time to replenish. • Each subsequent use of the stimulant will require higher and higher amounts to give the same effect. This is called tolerance. • During the time needed for the dopamine receptor to normalize, craving will occur.
Methamphetamine • Methamphetamine in particular causes the worse cravings. • This drug “upregulates the dopamine receptor” so high that with regular use of high amounts, the dopamine receptor actually dies creating black dots on a MRI scan. • These dots are dead brain tissue that will not regenerate. • The post-acute withdrawal syndrome for stimulants is at least as severe as opiates and alcohol.
Hallucinogens • The most commonly used hallucinogens are “shrooms” (mushrooms) and a variety of psychedelic drugs called “LSD”. • Most users get high and have distortions of senses such that they can hear colors or see music. • The problem is if they have a bad “trip” and end up having flashbacks of the bad trip with feelings of terror. • Some have committed suicide during these experiences.
Hallucinogens continued • “Spice” is supposed to be synthetic marijuana and “Bath Salts” is supposed to be like a stimulant. • Both are made up in someone’s bathroom sink and can be toxic causing auditory and visual hallucinations and paranoia requiring inpatient hospitalization.