Download
1 / 1

E N D
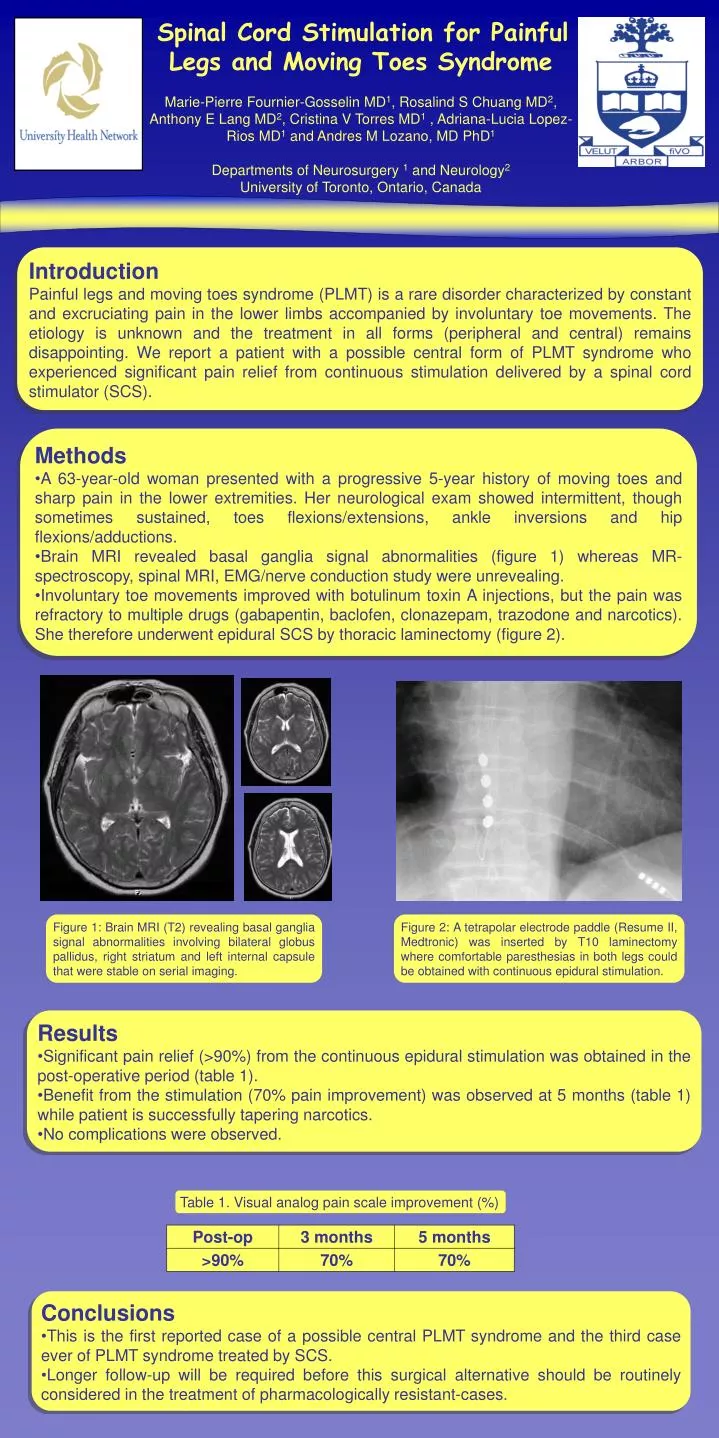
Spinal Cord Stimulation for Painful Legs and Moving Toes SyndromeMarie-Pierre Fournier-Gosselin MD1, Rosalind S Chuang MD2, Anthony E Lang MD2, Cristina V Torres MD1 , Adriana-Lucia Lopez-Rios MD1 and Andres M Lozano, MD PhD1Departments of Neurosurgery 1 and Neurology2University of Toronto, Ontario, Canada Introduction Painful legs and moving toes syndrome (PLMT) is a rare disorder characterized by constant and excruciating pain in the lower limbs accompanied by involuntary toe movements. The etiology is unknown and the treatment in all forms (peripheral and central) remains disappointing.We report a patient with a possible central form of PLMT syndrome who experienced significant pain relief from continuous stimulation delivered by a spinal cord stimulator (SCS). • Methods • A 63-year-old woman presented with a progressive 5-year history of moving toes and sharp pain in the lower extremities. Her neurological exam showed intermittent, though sometimes sustained, toes flexions/extensions, ankle inversions and hip flexions/adductions. • Brain MRI revealed basal ganglia signal abnormalities (figure 1) whereas MR-spectroscopy, spinal MRI, EMG/nerve conduction study were unrevealing. • Involuntary toe movements improved with botulinum toxin A injections, but the pain was refractory to multiple drugs (gabapentin, baclofen, clonazepam, trazodone and narcotics). She therefore underwent epidural SCS by thoracic laminectomy (figure 2). Figure 1: Brain MRI (T2) revealing basal ganglia signal abnormalities involving bilateral globus pallidus, right striatum and left internal capsule that were stable on serial imaging. Figure 2: A tetrapolar electrode paddle (Resume II, Medtronic) was inserted by T10 laminectomy where comfortable paresthesias in both legs could be obtained with continuous epidural stimulation. • Results • Significant pain relief (>90%) from the continuous epidural stimulation was obtained in the post-operative period (table 1). • Benefit from the stimulation (70% pain improvement) was observed at 5 months (table 1) while patient is successfully tapering narcotics. • No complications were observed. Table 1. Visual analog pain scale improvement (%) • Conclusions • This is the first reported case of a possible central PLMT syndrome and the third case ever of PLMT syndrome treated by SCS. • Longer follow-up will be required before this surgical alternative should be routinely considered in the treatment of pharmacologically resistant-cases.






