Download
1 / 1
20 likes | 84 Views
Elevated Slope Phase III from UPG correlates with intra-breath changes in low frequency reactance (X5Hz) in patients with COPD. Gary Nolan, Kristin A Southwell, Peter D Rochford, & Christine F McDonald

E N D
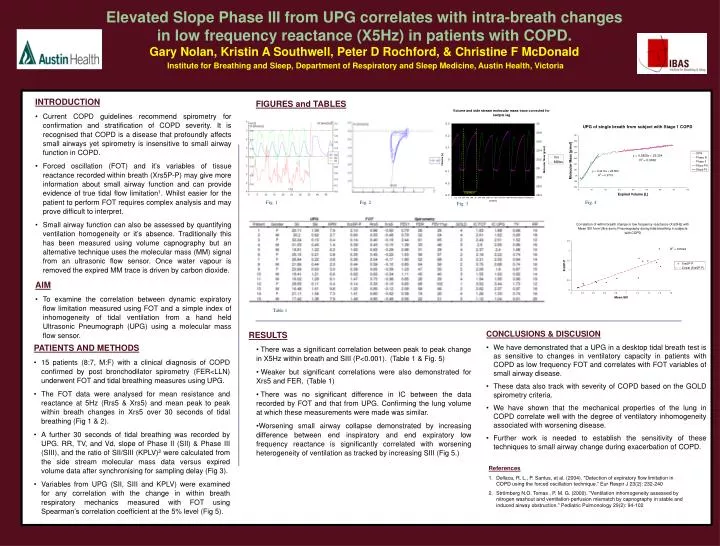
Elevated Slope Phase III from UPG correlates with intra-breath changes in low frequency reactance (X5Hz) in patients with COPD. Gary Nolan, Kristin A Southwell, Peter D Rochford, & Christine F McDonald Institute for Breathing and Sleep, Department of Respiratory and Sleep Medicine, Austin Health, Victoria • INTRODUCTION • Current COPD guidelines recommend spirometry for confirmation and stratification of COPD severity. It is recognised that COPD is a disease that profoundly affects small airways yet spirometry is insensitive to small airway function in COPD. • Forced oscillation (FOT) and it’s variables of tissue reactance recorded within breath (Xrs5P-P) may give more information about small airway function and can provide evidence of true tidal flow limitation1. Whilst easier for the patient to perform FOT requires complex analysis and may prove difficult to interpret. • Small airway function can also be assessed by quantifying ventilation homogeneity or it’s absence. Traditionally this has been measured using volume capnography but an alternative technique uses the molecular mass (MM) signal from an ultrasonic flow sensor. Once water vapour is removed the expired MM trace is driven by carbon dioxide. • AIM • To examine the correlation between dynamic expiratory flow limitation measured using FOT and a simple index of inhomogeneity of tidal ventilation from a hand held Ultrasonic Pneumograph (UPG) using a molecular mass flow sensor. FIGURES and TABLES Fig. 1 Fig. 2 Fig. 4 Fig. 3 Table 1 • CONCLUSIONS & DISCUSION • We have demonstrated that a UPG in a desktop tidal breath test is as sensitive to changes in ventilatory capacity in patients with COPD as low frequency FOT and correlates with FOT variables of small airway disease. • These data also track with severity of COPD based on the GOLD spirometry criteria. • We have shown that the mechanical properties of the lung in COPD correlate well with the degree of ventilatory inhomogeneity associated with worsening disease. • Further work is needed to establish the sensitivity of these techniques to small airway change during exacerbation of COPD. • RESULTS • There was a significant correlation between peak to peak change in X5Hz within breath and SIII (P<0.001). (Table 1 & Fig. 5) • Weaker but significant correlations were also demonstrated for Xrs5 and FER, (Table 1) • There was no significant difference in IC between the data recorded by FOT and that from UPG. Confirming the lung volume at which these measurements were made was similar. • Worsening small airway collapse demonstrated by increasing difference between end inspiratory and end expiratory low frequency reactance is significantly correlated with worsening heterogeneity of ventilation as tracked by increasing SIII (Fig 5.) PATIENTS AND METHODS • 15 patients (8:7, M:F) with a clinical diagnosis of COPD confirmed by post bronchodilator spirometry (FER<LLN) underwent FOT and tidal breathing measures using UPG. • The FOT data were analysed for mean resistance and reactance at 5Hz (Rrs5 & Xrs5) and mean peak to peak within breath changes in Xrs5 over 30 seconds of tidal breathing (Fig 1 & 2). • A further 30 seconds of tidal breathing was recorded by UPG. RR, TV, and Vd, slope of Phase II (SII) & Phase III (SIII), and the ratio of SII/SIII (KPLV)2 were calculated from the side stream molecular mass data versus expired volume data after synchronising for sampling delay (Fig 3). • Variables from UPG (SII, SIII and KPLV) were examined for any correlation with the change in within breath respiratory mechanics measured with FOT using Spearman’s correlation coefficient at the 5% level (Fig 5). • References • Dellaca, R. L., P. Santus, et al. (2004). "Detection of expiratory flow limitation in COPD using the forced oscillation technique." Eur Respir J 23(2): 232-240 • Strömberg N.O. Tomas , P. M. G. (2000). "Ventilation inhomogeneity assessed by nitrogen washout and ventilation-perfusion mismatch by capnography in stable and induced airway obstruction." Pediatric Pulmonology 29(2): 94-102






