Download
1 / 63
870 likes | 2.78k Views
Hemorrhagic Stroke. Lourdes James MS ACNP-BC CCRN The Johns Hopkins Hospital AACN Progressive Care Pathways Conference September 2013. Learning Outcomes. Identify the risk factors of hemorrhagic stroke Describe the etiology of hemorrhagic stroke

E N D
Hemorrhagic Stroke Lourdes James MS ACNP-BC CCRN The Johns Hopkins Hospital AACN Progressive Care Pathways Conference September 2013
Learning Outcomes • Identify the risk factors of hemorrhagic stroke • Describe the etiology of hemorrhagic stroke • Relate the pathophysiological processes of hemorrhagic stroke to progressive care patient pathways and nursing care
Stroke Definitions • Stroke • Any damage to brain or CNS structures caused by abnormalities of the blood supply • Acute-onset of symptoms • Cerebrovascular Accident (CVA) • More general term • Does not define time (acute/chronic) in relation to brain injury
Stroke Classification • Ischemic • 87% of all strokes • Hemorrhagic • Intracerebral Hemorrhage (ICH) – 10 to 15% of all strokes • Subarachnoid Hemorrhage (SAH) – 3% • Intraventricular Hemorrhage (IVH) • Rarely isolated • Typically extension of ICH • Occurs in 45% of patients with spontaneous ICH
ICH: Definition • Non-traumatic, abrupt onset of severe headache, altered level of consciousness, or focal neurological deficit associated with a focal collection of blood within the brain parenchyma which is not due to trauma or hemorrhagic conversion of a cerebral infarction
ICH: Epidemiology • Incidence rates in Western Hemisphere • 10 – 30 cases/100,000 • Incidence rates are higher in Eastern Asia • Incidence greater in men than women
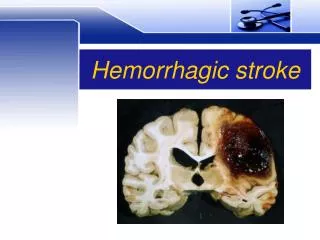
ICH: Location • Location varies in populations • Deep cerebral hemorrhage • Most common in US, Europe and Australia • Lobar hemorrhages • Second to deep cerebral hemorrhage • ≅15% of ICHs • Cerebellar hemorrhages • ≅10% of ICHs • Brainstem hemorrhages • ≅5 – 10% of ICHs
A: Lobar: originating from penetrating cortical branches of the anterior, middle, or posterior cerebral arteries B: Basal ganglia: originating from ascending lenticulostriate branches of the middle cerebral artery C: Thalamus: originating from ascending thalmogeniculate branches of the posterior cerebral artery D: Pons: originating from paramedian branches of the basilar artery E: Cerebellum: originating from penetrating branches of the posterior inferior, anterior inferior, or superior cerebellar arteries
ICH: Risk factors • Hypertension • Age • Race • Cerebral Amyloid Angiopathy • Aneurysms/Vascular Malformations • Apolipoprotein E and CAA • Anticoagulants/Thrombolytics • Antiplatelets • Cerebral Microbleeds • Prior Cerebral Infarction • Hypocholesterolemia • Heavy Alcohol Use • Tobacco Use • Diabetes • Heritability
ICH: Etiology • Hypertension • IVDA/Cocaine Use • Vascular malformations • AVM • Aneurysm • Cavernous angioma • Amyloid angiopathy • Coagulopathies • Neoplasm • Trauma
ICH: Pathophysiology • Damage to small penetrating arteries and arterioles (HTN) • Rupture of small penetrating arteries • Local pressure effect on surrounding capillaries and arterioles • Accumulation of hematoma
ICH: Clinical Presentation • Severe headache • Focal neurological deficits • Coma or decreased LOC • SBP > 200 mmHg • Vomiting • Given that symptoms are non-specific, • neuroimaging is a necessity
ICH: Neuroimaging • CT or MRI to distinguish between ischemic or hemorrhagic stroke • Hematoma expansion? • CTA or contrast-enhanced CT • Underlying structural lesions? • CTA/CTV, contrast-enhanced CT, contrast-enhanced MRI, MRA/MRV • Underlying vascular anomaly? • Cerebral angiography if high suspicion
ICH: Symptom Progression • Worsening of symptoms during first 24 – 48 hours: • Continuation of bleeding • Hematoma enlargement • Cerebral edema • Herniation
ICH: Hematoma Expansion • High rate of early neurologic deterioration due to bleeding occurring for hours after symptom onset • Head CT within 3 hours after symptom onset: • 28 – 38% have hematoma expansion of > 1/3 • Predictive of neurologic deterioration and increased morbidity and mortality
ICH: Inpatient Management • Obtain Hemostasis • Severe coagulation factor deficiency or thrombocytopenia • Replace factors and/or platelets • If INR elevated due to oral anticoagulation: • Hold warfarin (Coumadin) • Replace Vitamin K dependent factors (IV Vitamin K recommended) • Correct INR
ICH: Inpatient Management • General Monitoring • Initial monitoring in ICU • Blood Pressure (BP) Management • Incomplete efficacy evidence at present until ongoing trials of BP intervention • Patients with Systolic BP (SBP) 150 – 220mmHg, acute lowering to SBP < 140mmHg probably safe (Class IIa, Level B)
ICH: Inpatient Management • Temperature Management • Duration of fever linked to outcome, prognostic factor in patients surviving first 72H • Maintain normothermia • Seizure Prophylaxis • Treat with anti-epileptic drugs (AED) for patients with clinical seizures, electrographic seizures + change in MS • Prophylaxis with AED not recommended (Class III, Level B)
ICH: Inpatient Management • Glycemic Control • Maintain normoglycemia • DVT prophylaxis • Intermittent pneumatic compression + elastic stockings • May consider low-dose LMWH after ICH stability established and 1-4 days from onset (Class IIb, Level B)
ICH: Inpatient Management • Code Status • Aggressive full care early after ICH onset • Postponement of new DNR orders until at least the second full day of hospitalization is probably recommended (Class IIa,Level B) • Does not include patients with pre-existing DNR status
ICP Monitoring & Treatment • ICP Monitoring Indications (Class IIb, Level C) • GCS ≤ 8 • Transtentorial herniation • Significant IVH or hydrocephalus • CPP of 50 – 70 mmHg (Class IIb, Level C) • Ventricular drainage reasonable for treatment of hydrocephalus in patients with decreased LOC (Class IIa, Level B)
ICH: Surgical Interventions • Indications for Surgical Removal of Hemorrhage • Usefulness of surgery uncertain (Class IIb, Level C) • Cerebellar hemorrhage with evidence of neurological deterioration, or brain stem compression, and/or hydrocephalus (Class I, Level B) • Lobar clots > 30mL and within 1 cm of surface, supratentorial clot evacuation via craniotomy may be considered (Class IIb, Level B)
ICH: Recurrence Prevention • BP Management • BP should be well-controlled after acute ICH • BP <140/90mmHg, <130/90mmHg if DM or CKD (Class IIa, Level B) • Anticoagulation • Avoid long-term anticoagulation for non-valvular atrial fibrillation after lobar ICH (Class IIa, Level B) • Anticoagulation after non-lobar ICH and anti-platelet therapy after all ICH might be considered when definite indication (Class IIB, Level B)
ICH: Recurrence Prevention • Avoidance of heavy alcohol usage (Class IIa, Level B) • Insufficient data to recommend restrictions for: • Statins • Physical activity • Sexual activity
ICH: Nursing Considerations • Neurological monitoring • Change in exam? • Hematoma expansion? • Worsening cerebral edema/herniation? • Increased ICP? • Seizure? • ICP/Cerebral perfusion pressure (CPP) monitoring • BP management and hemodynamic monitoring • Airway maintenance • Maintain normothermia • Maintain normoglycemia • Prevention of complications
Subarachnoid Hemorrhage (SAH) • Bleeding into the subarachnoid space (between the arachnoid layer and pia mater)
SAH: Etiology • Trauma • Most common • Ruptured cerebral aneurysm • Most described in literature • Aneurysmal subarachnoid hemorrhage (aSAH)
aSAH: Epidemiology • US incidence: 9.7/100,000 • 14.5 discharges/100,000 • US mean mortality rate: 32% • Death occurs in 12-15% of cases before reaching hospital • True incidence may be higher? • Average age of onset ≥ 50 • Incidence higher in females than males • African Americans and Hispanics have higher incidence
aSAH: Behavioral Risk Factors • Hypertension • Tobacco Use • Alcohol Abuse • Sympathomimetic drugs (cocaine)
aSAH: Non-modifiable Risk Factors • Female gender • Unruptured aneurysm • Symptomatic • Larger in size • Posterior communicating artery or vertebrobasilar location • Previous aSAH • Familial aneurysms • At least 1 first-degree relative, especially ≥ 2 first degree relatives • Genetic syndromes
aSAH: Clinical Presentation • “Worst headache of life” • Described by ≈ 80% of patients • Onset of headache may be associated with: • Nausea • Vomiting • Nucchal rigidity • Photophobia • Focal neurological deficits • Loss of consciousness
aSAH: Diagnosis • Clinical presentation • High level of suspicion with acute onset severe headache • Neuroimaging • CT for suspected SAH • Lumbar Puncture (LP) if CT negative • CTA may be used to detect aneurysm • if inconclusive, will need cerebral angiogram • Cerebral angiography for +SAH to identify presence of aneurysm if not detected on noninvasive angiogram • MRI may be reasonable for diagnosis, would still need LP
aSAH: Prognosis • SAH Grading Scales • Hunt and Hess Scale • Fisher Scale • Degree of neurological impairment associated with prognosis
aSAH: Prevention of Rebleed • BP Management (SBP < 160mmHg) • Bedrest • Antifibrinolytic therapy? • For patients with unavoidable delay in surgical/endovascular treatment • < 72 hours of therapy • tranexamic acid or aminocaproic acid is reasonable
aSAH: Prevention of Rebleed • Surgical/endovascular treatment of ruptured aneurysm • Surgical clipping of cerebral aneurysm • Stent/coiling of cerebral aneurysm • Should be performed as early as possible • Complete obliteration recommended
aSAH: Complications • Cerebral Vasospasm and Delayed Cerebral Ischemia (DCI) • Hydrocephalus • Hyponatremia and Volume Contraction • Seizures • Cerebral edema • Rebleed • Neurogenic Stress Cardiomyopathy