Download

1 / 41
420 likes | 1.11k Views
Contraceptive Methods. Spacing Methods. Barrier Methods: a. Natural methods b. Physical methods c. Chemical methods d. Combined Methods 2. Intra-Uterine Devices 3. Hormonal Methods 4. Post- Conceptional Methods 5. Miscellaneous. Natural methods. Coitus interruptus

E N D
Spacing Methods • Barrier Methods: • a. Natural methods b. Physical methods c. Chemical methods d. Combined Methods 2. Intra-Uterine Devices 3. Hormonal Methods 4. Post-Conceptional Methods 5. Miscellaneous
Natural methods • Coitus interruptus • Rhythm method or safe period methods • This method is to abstain from sex during fertile period. • Temperature change method • The basal body temp in a fertile women rises by 0.4 to 1.0 F during ovulation. • Lactation Ammenorrhea method • Exclusive breast feeding in Lactation Ammenorrhea offers saves from pregnancy
Physical methods: Condoms & Diaphragm Advantages: • Easily available • Safe and inexpensive • Easy to use • No side effects • Light, compact and disposable • Provides protection against STDs & cervical cancer Disadvantages: • It may slip off or tear during coitus due to incorrect use, • Interferes with sex sensation locally • Can cause irritation or allergic reaction.
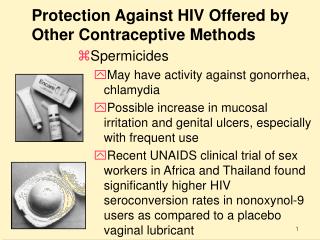
Chemical methods • Vaginal spermicidal agents • Failure rate of spermicides when used alone is 10 to 20 percent. • Vaginal contraceptive sponge • ‘Today’ is the name given to vaginal contraceptive sponge available in USA and UK.
Intra-Uterine Devices • IUD is a device based on spacing method of contraception , requiring one time insertion procedure and is effective for long duration • ( 3-10 yrs depending on the type of IUD used).
IUCDs • Types of IUCD • Non-medicated: • Lippies loop, spirals, coils, rings • Medicated: • Copper, silver core, Multi load Devices • Release of hormones • Progestasert • Levonorgestril
Action of IUCDs • Foreign body, cellular and biochemical changes in endometrium - impair viability of gametes • Hormone releasing devices increase viscosity of the cervical mucus • High level of progesterone – unfavorable for implantation.
Advantages of IUCDs • Most effective method • Simple, in a few minutes • Long acting, may be for 5-10 years • Inexpensive • Reversible • Lower incidence of side-effects, free of metabolic side effects
Advantages of IUCDs • Highest continuation rate • No need for continued motivation • Easier to fit even in nulli parous women • Better tolerated by nulli para • Effective as post-coital contraceptive
Mechanism of action of IUCDs • At present, the most widely accepted view is that the IUCD causes a foreign-body reaction in the uterus causing cellular and biochemical changes in the endometrium and uterine fluids, and it is believed that these changes impair the viability of the gamete and thus reduce its chances of fertilization, rather than its implantation.
ABSOLUTE C/I OF IUCDs • Suspected pregnancy • Pelvic inflammatory diseases • Vaginal bleeding of undiagnosed aetiology • Cancer of the cervix, uterus or adnexia • Previous Ectopic pregnancy
RELATIVE C/I OF IUCDs • Anaemia • Menorrhagia • H / O PID since last pregnancy • Purulent cervical discharge • Malformations, • Fibroids • Unmotivated client or person
The ideal IUD candidate • Who has borne at least one child • Has no history of pelvic disease • Has normal menstrual periods • Is willing to check the IUD tail • Has access to follow-up and treatment of potential problems
TIME OF INSERTION OF IUCD • Any time during reproductive age • During menstruation or within 10 days of the beginning of menstrual cycle • First week after delivery-immediate postpartum insertion • Better time is at 6-8 weeks after delivery-post puerperal insertion
Side effects of IUCD • 1. Bleeding, greater loss, prolonged period • 2. Pain • 3. Pelvic infection • 4. Uterine perforation • 5. Pregnancy • 6. Ectopic pregnancy • 7. Expulsion • 8. Fertility after removal • 9. Cancer and teratogenesis • 10. Mortality
HORMONAL CONTRACEPTIVES • Most effective spacing method • 100% effective • Synthetic estrogens • Ethinyl oestradiol • Mestranol • Synthetic progesterone • Pregnanes • Oestranes • Gonanes
Classifications A. Oral Pills 1. Combined pill 2. Progestogen only pills (POP) 3. Post-coital pills 4. Once-a-month (long-acting) pill 5. Male pills B. Depot (slow release) formulations 1. Injectables 2. Subcutaneous implants 3. Vaginal rings
Combined pills • Major spacing method • 30-35 microgram of synthetic estrogen • 0.5-1.0 microgram of progestogen. • Pill is given orally for 21 consec. Days, starting on 5th day of menstrual cycle • Pill is taken every day at a fixed time
POP • Contains only progesterone • Small doses throughout the cycle • For those women- c/I combined pills
Post coital contraception • Morning after • Within 48 hours of unprotected intercourse • IUCD • Hormonal: high doses of estrogen and progesterone • 2 pills immediately & 2 pills after 12 hours
Once a month pill • Long acting estrogen • Short acting progesterone
Mode of action of OCP • Prevents the release of ovum from ovary by locking pituitary secretion of gonadotropin. • Progesterone only pills renders the mucus thick, scanty that inhibits sperm penetration. • Progesterone also inhibits tubal motility • OCP are 100 % effective if taken regularly • Certain drugs affects the effect of OCP
Beneficial effects • 100 % effective contraception • Protection against • Benign breast disorders • Ovarian cysts • Iron deficiency anaemia • PID • Ectopic pregnancy • Ovarian cancer
Adverse effects of OCP • Cardiovascular effects • Carcinogens • Metabolic effects • Elevation of BP, decrease in high density lipoprot. • Blood clotting, increase sugar level • Increase in atherogenesis • Increase in myocardial infarction & stroke • Others: • Liver disorder, lactation, fertility, ectopic preg. • Breast tenderness, weight gain, headache, • Bleeding disturbances , Foetal development
Contraindications of OCP • Cancer of breast & genitals • Liver disease • Cardiac diseases, DVT • Congenital hyperlipideamia • Undiagnosed abnormal uterine bleeding • Age above 40 & smoker at age 35 • Hypertension, migraine, headache, epilepsy, diabetes, gall bladder disease • Nursing mother in first 6 months
Checklist for Oral Contraceptives • Above 40 years of age • Above 35 years of age & heavy smoker • H / O Seizures • Severe pain in the calves or thighs • Symptomatic varicose veins in the legs • Severe chest pains, shortness of breath • Severe headache • Visual problems
Lactating less than 6 months • Inter menstrual bleeding • Bleeding after sexual intercourse • Amenorrhoea • Abnormally yellow skin & eyes • High Blood pressure • Mass in the breast • Oedema - legs
Depot formulations • Injectables: • DMPA 150 mg every 3 months • 99%, safe, effective, acceptable during lactation • Wt. gain, irregular menstrual bleeding • prolonged infertility • NET-EN 300 mg 2 months • Inj. During first 5 days of menstruation • Deep intramuscular into gluteus maximus. • Never massage • ± 2 weeks
Depot formulations • Sub dermal implants • Norplant • 6 silicone rubber capsules containing 35 mg of Levonorgestril • Implanted under the skin of left upper arm
Terminal Methods • Permanent methods • Male sterilization • Female sterilization • Females 90 – 95% • Males 5 – 10% • One time method, no sustained motivation • Risk of complications is rare
Male sterilization: Vasectomy Post-operative advice • Patient is not sterile immediately after the operation • At least 30 ejaculations may be necessary before the seminal examination is negative • To use contraceptives until aspermia has been established • To avoid taking bath for at least 24 hours after the operation. • To wear a T-bandage or scrotal support for 15 days and to keep the site clean and dry • To avoid cycling or lifting heavy weights for 15 days • Remove stitches on the 5th day after the operation.
COMPLICATIONS • Operative • Sperm granules • Spontaneous reorganization • Autoimmune response • Psychological
Female sterilization:Bilateral Tubal Ligation (BTL) • It is the most widely used contraceptive method. The procedure can be carried out in the immediate post menstrual and post partum period. • Laparoscopic sterilization is most commonly employed method. • Failure and complications only due to surgical skills.
MCQ • Thread attached with IUCD is meant for • Anti inflammatory effect • Device can be pulled out when needed • Shape of loop • Assurance of loop’s presence • Blocking of sperm penetration
MCQ • Multi load contains • Copper • Zinc • Silver • Gold • Progesterone
MCQ • OCP is not c/I in • Pregnancy • Lactation • Fibroid • Overweight • A woman having 2-3 children
MCQ • Most effective contraceptive method for spacing between pregnancies is • IUCD • Oral pills • Condom • Vasectomy • Abstinence from sexual intercourse
MCQ • Estrogen content of OCP causes all except: • Myocardial infarction • Venous thrombo - embolism • Decreased quantity of breast milk • Increased blood sugar • Breast tenderness