Download
1 / 31

E N D
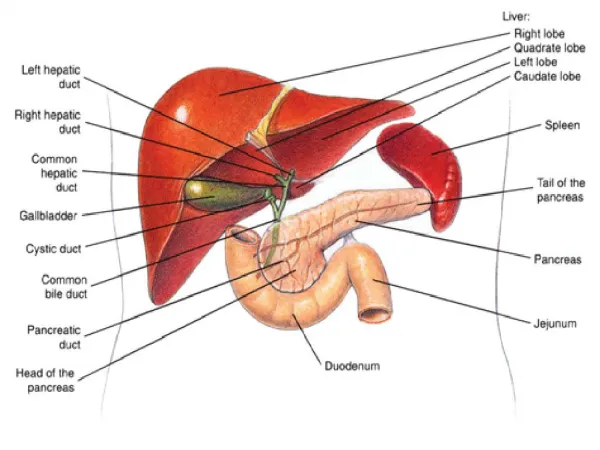
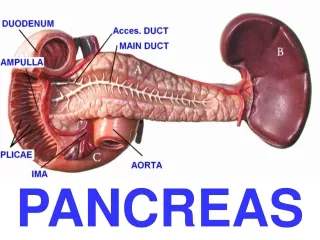
1. Pancreas
2. Pancreas
3. Pancreas Pancreatic acini,
radial orientation of the pyramidal exocrine acinar cells.
cytoplasm is for the synthesis and packaging of digestive enzymes for secretion into a central lumen
4. Pancreas
Congenital anomalies:
1.Agenesis = incompatible with life
2. Pancreas Divisum = persistence as dorsal and ventral pancreas
Predisposes to Chronic Pancreatitis
3. Annular pancreas = pancreatic head encircles the duodenum
Risk of Intestinal obstruction
4. Aberrant (or Ectopic) pancreas = located in the stomach, SI, Meckel�s Diverticulum, submucosal, yellow-gray nests
5. Pancreas - Pancreas Divisum
6. Pancreas - Annular pancreas
7. Pancreas
Acute Pancreatitis= acute abdominal pain, radiating to the back
Types
Acute interstitial pancreatitis= Mild form with edema
Acute necrotizing pancreatitis = Severe pancreatitis with tissue necrosis
Acute hemorrhagic pancreatitis = Most severe form with extensive hemorrhage
raised levels of pancreatic enzymes (amylase and lipase) in Blood or Urine
MCC= cholelithiasis and alcoholism
Alcohol = proposed mechanism of acinar cell injury
misdirected intracellular transport of Proenzymes
protein plugs within pancreatic ducts,
local obstruction and inflammation
Clinical
Medical emergency with acute abdomen,
constant and intense abdominal pain with upper back radiation,
peripheral vascular collapse and shock
Death occurs from shock, ARDS, Acute renal failure
8. Pancreas
Acute Pancreatitis
Lab findings
first 24 hours -marked elevation of the serum amylase
within 72 to 96 hours -rising serum lipase,
Glycosuria occurs in 10% of cases,
Hypocalcemia, if persistent- poor prognostic sign
Complications
pancreatic abscess
Pseudocyst
9. Acute Pancreatitis Microscopic field shows a region of fat necrosis on the right
10. Pathways of Acute pancreatitis
11. Acute Pancreatitis hemorrhage in the head of the pancreas
fat necrosis
12. Pancreas
Chronic Pancreatitis= Repeated bouts pancreatitis with loss of pancreatic parenchyma & pancreatic function
Replacement by fibrous tissue (islets of Langerhans are spared)
Causes
Ductal obstruction by concretions (as with alcohol)
decreased acinar secretion of lithostatine (inhibit intraluminal precipitation of calcium carbonates)
Complications
Pseudocyst
diarrhea (malabsorption)
diabetes
13. Chronic Pancreatitis A, Extensive fibrosis and atrophy has left only residual islets (left) and ducts (right), with a sprinkling of chronic inflammatory cells and acinar tissue.
B, A higher-power view demonstrating dilated ducts with inspissated eosinophilic ductal concretions in a patient with alcoholic chronic pancreatitis.
14. Sequelae of Acute and Chronic Pancreatitis
15. Pancreatitis
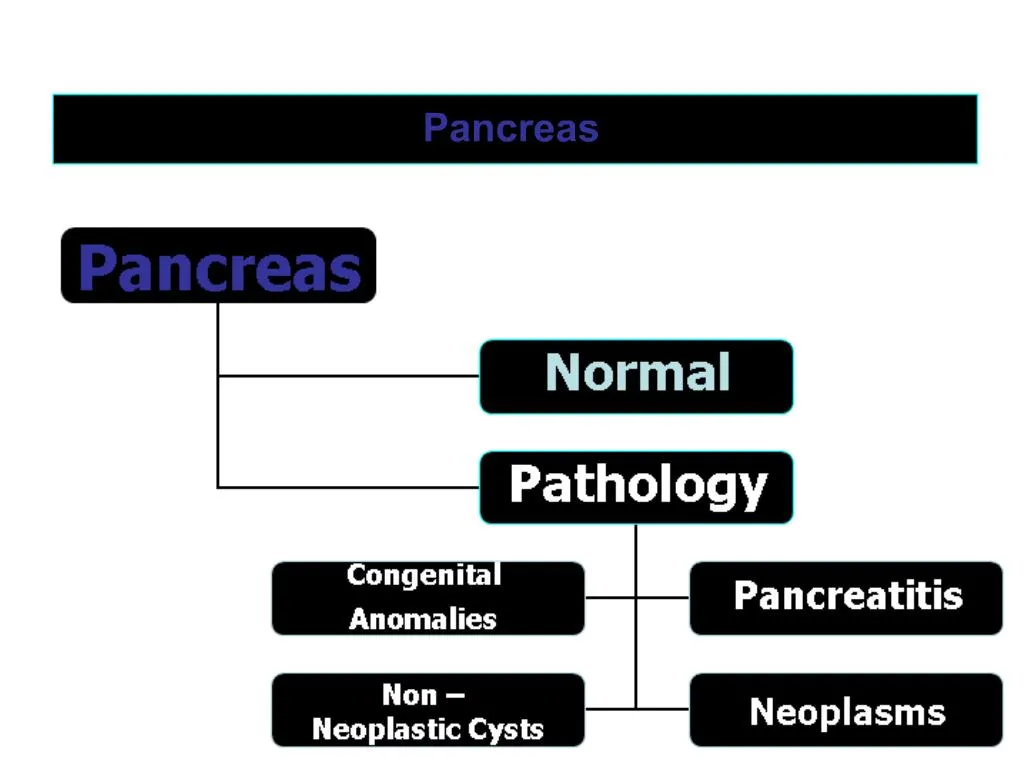
16. Pancreas
Pancreatic Cysts
Non-neoplastic =MC (75%) �Pseudocyst (Acquired)
Complication after acute or chronic pancreatitis,
Unilocular cyst, no epithelial lining
Congenital =Part of Poly cystic disease
congenital polycystic disease =coexist with kidney and liver cysts
Neoplastic
Benign � Unilocular
Malignant � Multilocular
Von-Hippel-Lindau disease = Congenital pancreatic cysts and angiomas of the CNS (Retina, Cerebellum)
17. Cystic Neoplasms
19. Unilocular Vs Multilocular cysts
20. Pancreatic pseudocyst A, Cross-section through this previously bisected lesion revealing a poorly defined cyst with a necrotic brown-black wall.
B, Histologically, the cyst lacks a true epithelial lining and instead is lined by fibrin and granulation tissue
21. Serous cystadenoma A, Cross-section through a serous cystadenoma. Only a thin rim of normal pancreatic parenchyma remains. The cysts are relatively small and contain clear, straw-colored fluid.
B, The cysts are lined by Cuboidal epithelium without atypia.
22. Mucinous Cystic Tumor A, Cross-section through a mucinous multiloculated cyst in the tail of the pancreas. The cysts are large and filled with tenacious mucin.
B, The cysts are lined by columnar mucinous epithelium, and a dense "ovarian� like stroma is noted
23. 3. Intraductal papillary Mucinous Neoplasm A, Cross-section through the head of the pancreas showing a prominent papillary neoplasm distending the main pancreatic duct.
B, The papillary mucinous neoplasm involved the main pancreatic duct (left) and extending down into the smaller ducts and ductules (right).
24. Pancreas
Carcinoma Pancreas = carcinomas of the exocrine pancreas
5% of all cancer deaths in the US at age of 60 and 80�s
arising from ductal epithelial cells,
? incidence in smokers and alcoholics
Genetics
K-ras mutations in 90% cases (MC altered oncogene)
p53 mutations in 60 to 80% cases
P16- MC inactivated tumor suppressor gene
Site= MC in in the head (60%)
Microscopically = (adenocarcinoma-MC type)
Prognosis
five-year survival - 5%
25. Pancreas
1.Carcinoma Pancreas
first year mortality >80%,
Clinically
weight loss, pain & obstructive jaundice
massive metastasis to the liver occurs via splenic vein invasion,
migratory thrombophlebitis (Trousseau syndrome)
Biochemical tests = Carcinoembryonic antigen (CEA) and CA19-9 antigen
Diagnosis= endoscopic ultrasonography and CT& FNAC
2. Pancreatoblastoma =rare neoplasms in children, fully malignant
3. Periampullary carcinomas = pancreatic carcinomas at ampulla of Vater
85% are unresectable at presentation,
26. Carcinoma - Pancreas
27. Carcinoma - Pancreas A, A cross-section through the head of the pancreas and adjacent common bile duct showing both an ill-defined mass in the pancreatic substance (arrowheads) and the green discoloration of the duct resulting from total obstruction of bile flow.
B, Poorly formed glands are present in densely fibrotic stroma within the pancreatic substance; there are some inflammatory cells
28. Case A 40-year-old woman developed increasingly severe abdominal pain over a two day period. In the emergency room, physical examination demonstrated board-like rigidity of her abdomen along with extreme tenderness. A plain film radiograph of the abdomen demonstrated dilated loops of bowel, several radiopaque gallstones in the gallbladder, but no free air. The total bilirubin was 3.8 mg/dL, AST 25 U/L, ALT 30 U/L, albumin 3.5 g/dL, total protein 5.8 g/dL, glucose 120 mg/dL, calcium 7.8 mg/dL, phosphorus 3.3 mg/dL, and lipase 2,250 U/L. The gross photograph depicts the process (image 7.1). The microscopic appearance is seen in images 7.2 and 7.3.
29. Case
30. Case
31. Case -1