Download
1 / 18
190 likes | 316 Views
WHAT PATHOLOGY TESTS TO ORDER WHEN A PATIENT PRESENTS WITH ATYPICAL PNEUMONIA. Stephen GRAVES Director Division of Microbiology. How does “atypical pneumonia” differ from “typical pneumonia” slower onset of symptoms (days rather than hours) – longer prodrome.

E N D
WHAT PATHOLOGY TESTS TO ORDER WHEN A PATIENT PRESENTS WITH ATYPICAL PNEUMONIA Stephen GRAVES Director Division of Microbiology
How does “atypical pneumonia” differ from “typical pneumonia” • slower onset of symptoms (days rather than hours) – longer prodrome. • less prominent respiratory symptoms • less/no sputum • less chest pain • less dyspnoea • normal FBC (WCC not raised) • “normal” CXR (non-lobar changes) [ treat with doxycycline/clarithromycin/azithromycin rather than benzypenicillin/amoxycillin]
Causes of typical pneumonia • bacteria • Streptococcus pneumoniae • Haemophilus influenzae • Staphylococcus aureus • Klebsiella pneumoniae (and other Gram-negatives, especially in hospitalised and intubated patients) • rarely viral • Ix sputum (m/c/s) • blood cultures (x2)
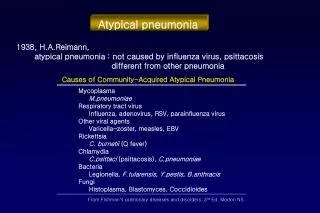
Causes of atypical pneumonia • Viruses • Influenza A • Rhinoviruses • Respiratory Syncytial Virus (RSV)
Causes of atypical pneumonia (cont.) Bacteria • Mycoplasma pneumoniae • Legionella sp. (cooling tower waters/potting mix) • Chlamydia pneumoniae • Chlamydia psittaci (bird contact) • Coxiella burnetii (Q fever) (animal contact) • Mycobacterium tuberculosis (immigrant) Fungi • Pneumocystis jiroveci (immunosuppressed/HIV)
Pathology investigations for atypical pneumonia Depends on what you think is the cause: • Baseline serology (may be negative, but can be used with a later serum to demonstrate seroconversion) e.g. Mycoplasma pneumoniae IgM and IgG. • Direct immunofluorescence (IF) on respiratory tract specimens (for respiratory viruses & Pneumocystis) • PCR on respiratory tract specimen (for respiratory viruses & Pneumocystis) [this is now replacing viral culture]
Pathology investigations for atypical pneumonia (cont.) • Legionella Urinary antigen (for L.pneumophila serogroup1 only) • Q Fever PCR/serology • Culture of respiratory tract specimens for bacteria • Consider tests for TB in risk groups
WHAT PATHOLOGY TESTS TO ORDER WHEN PATIENT PRESENTS WITH JAUNDICE/HEPATITIS Stephen GRAVES Director Division of Microbiology
INFECTIOUS CAUSES • viral hepatitis (many possibilities) • bacterial • septicaemia • cholangitis/cholecystitis • pyogenic liver abscess • peritonitis • rare infections • malaria (travellers) • amoebic liver abscess • leptospirosis • Q fever • brucellosis • hydatid cyst } animal contact
OTHER NON-INFECTIOUS CAUSES OF PATHOLOGY • drug-induced (including alcohol) • neoplasia (liver infiltration or biliary obstruction) • haemolysis
INVESTIGATIONS • Full blood examination (↑ eosinophils suggest parasite or drug-induced hepatitis) • Liver function tests • Blood cultures (x2) • Urinalysis • Viral serology (must specify which viruses) • Special tests • e.g. serology for specific infections • e.g. ascites fluid (m/c/s) base-line (acute) serum (will also be stored for later use) • if haemolysis, consider serology for • Mycoplasma pneumoniae & EBV
Viral causes of jaundice/hepatitis } • Epstein-Barr Virus (EBV) • Cytomegalovirus (CMV) • Hepatitis A (HAV) (travellers) • Hepatitis B (HBV) (ethnic risk, IVDU) • Hepatitis C (HCV) (IVDU) • Hepatitis D (HDV) (only if Hep B positive) • Hepatitis E (HEV) (travellers) The laboratory cannot test for all of these simultaneously! You must indicate which you think is most likely or indicate a descending order of probability (teenagers)
Investigations Baseline serology in acute illness (may be negative but can be used in conjunction with a later serum to demonstrate seroconversion or rise in antibody concentration/titre) • HAV serology (travellers, non-immunised) • IgM and IgG in acute illness • IgG only if testing for immunity or past infection
Investigations (cont.) • HBV serology (ethnic risk, IVDU) • HBVsAg – acute infection; chronic infection • HBVsAb – immunity (post-vaccination) • HBVcIgG – confirms prior infection • HBVcIgM – confirms recent infection • HBVeAg – high risk chronic infection • HBVeAb – past infection • HBV DNA - acute infection; chronic infection
Investigations • HCV serology • IgG – past infection or chronic infection • HCV – RNA – acute or chronic infection • HCV – RNA (viral load) – response to Rx? • HCV – genotype – is virus likely to respond to Rx? • genotype 1 (40% cure) • genotype 2/3 (80% cure)
Investigations • EBV serology • monospot/Paul-Bunnell test (heterophile antibody) • specific serology • EBV IgM acute infection • EBV IgG past infection • PCR (to detect DNA) acute/chronic/reactivation infection
Investigations • CMV specific serology • CMV IgM acute infection • CMV IgG past infection • PCR (to detect DNA) acute/chronic/reactivation infection
If in doubt what test to order, please phone the Duty Medical Microbiologist on Ext. 14000