Download
1 / 25
270 likes | 477 Views
End of Life planning: Beyond the DNR Order. Canadian Health Libraries Association 2012 Conference Alan Taniguchi, MD June 14, 2012. The Elephant in the Room By Terry Kettering. What I Hope to Accomplish. Write the great Canadian novel

E N D
End of Life planning:Beyond the DNR Order Canadian Health Libraries Association 2012 Conference Alan Taniguchi, MD June 14, 2012
The Elephant in the Room By Terry Kettering
What I Hope to Accomplish • Write the great Canadian novel • Read (and understand) Proust’s À la recherche du temps perdu • Start a conversation about the end of life • Discuss the role of advance care planning (ACP) • Offer ideas on how you can achieve what you want • Stimulate your thinking about death and dying
What I Hope to Accomplish Write the great Canadian novel Read (and understand) Proust’s Remembrance of Things Past • Start a conversation about the end of life • Discuss the role of advance care planning (ACP) • Offer ideas on how you can achieve what you want • Stimulate your thinking about death and dying
Our Last Phase of Life: A Century of Change 19002000 Age at death 46 years 78 years Top Causes Infection Cancer Accident Organ system failure Childbirth Stroke/Dementia Disability Not much 2-4 yrs before death Financing Private, Publicand substantial modest Joanne Lynn 2006
Sudden 7% Other 9% Cancer 22% Frail 46% Heart and Lung Failure 16% How Will We Die?
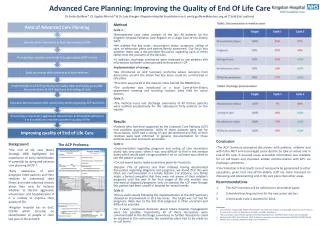
Theoretical Trajectories of Dying High High High High Function Function Function Function Low Low Low Low Time Time Time Time Sudden Death Terminal Illness Death Death Frailty Organ Failure Death Death Lunney JR, Lynn J, Hogan C. Profiles of older medicare decendents I Am Geriatr Soc. 2002; 50:1108-1112
Prognosis often uncertain, even late in life Severity of patient condition dictates needs Most patients need both disease-modifying treatments and help to live well with disease Triage Question of Choice for ACP Would you be surprised if this patient died in the next year, even with optimal treatment? If not – consider the need for advance care planning and palliative/hospice care. Severity of Illness, not Prognosis
Improving End-of-Life Care Proactive & Collaborative End-of-Life planning benefits patients: • Enables patients to avoid unwanted, invasive and futile treatments • Empowers patients/families by giving them choices (location of death, modes of treatment, etc.) • Supports holistic care (physical, emotional, spiritual) • Allows patients/families to express wishes, needs, values and to prepare for death
What Patients Want at EoL: The Evidence D.K. Heyland, et al; CMAJ (174): 2006 What do seriously ill patients (in hospital) and family consider key elements of quality end-of-life care? Interviews with 440 patients (advanced cancer or chronic end-stage medical disease) and 160 relatives Results: Patient perceptions of quality EoL care Trust & confidence in doctors To not be kept alive on life support if little hope for meaningful recovery Info about disease communicated honestly Opportunity to complete things, prepare for death To not be physical/emotional burden on family Clear discharge plan Relief of symptoms (pain, nausea, etc.)
What Families Want at EoL: The Evidence D.K. Heyland, et al; CMAJ (174): 2006 What do seriously ill patients (in hospital) and family consider key elements of quality end-of-life care? Interviews with 440 patients (advanced cancer or chronic end-stage medical disease) and 160 relatives Results: Family perceptions of quality EoL care Trust & confidence in doctors To not have patient kept alive on life support if little hope for meaningful recovery Info about patient’s disease communicated honestly Clear discharge plan for patient Patient receives relief of symptoms (pain, nausea, etc.) Opportunity to strengthen relationship with patient Info about patient’s illness and needs available Complete things, resolve conflicts, say goodbye to patient
New Ways of Speaking… AND, not DNR! S.S. Venneman, et al; Journal of Medical Ethics 34: 2008 Family members often misunderstand DNR as permission to terminate patient’s life: negative connotations Physicians and family fear abandonment of patient labeled DNR “Allow Natural Death” (AND): positive language that conveys the goal of treatment plan
Allow Natural Death... • Focus on what we are doing for the patient (“Allow Natural Death”) rather than what we are not doing (“Do Not Resuscitate”) • Instructs health care team to allow dying process to occur uninterrupted • A choice for quality care, respect & dignity provided to the patient: - pain & symptom management • spiritual & psychological support • additional medical interventions to support quality of life
Elderly patient admitted for planned surgery; EoL wishes discussed with physician, “no code” recorded in progress notes but no order written; patient arrests post-op, CPR initiated, admitted to ICU; family angry that patient’s wishes not honored; treatment eventually withdrawn in ICU. Patient identified as dying by staff; transferred to another floor; patient arrests after transfer; new staff can’t confirm code status; CPR initiated; DNR later located buried in the chart. Real Cases @ HHS 3. Patient with terminal illness asks staff to withdraw life-sustaining treatment; days later loses capacity to make treatment decisions; family refuses to believe staff, insist on continuing; treatment eventually withdrawn after weeks in ICU.
HHS Quality End-of-Life Initiative • Goals of the HHS QEoL Initiative: • Proactive identification of individuals at risk of death • Patient/family engagement in EOL conversations • Consistent documentation of EOL wishes • Collaborative team approach to care, aligned with patient wishes/values
POST – Physician Ordered Scope of Treatment • Has a red right side border for quick identification • MANDATORY placement at the front of the physician orders section in the chart • Transcribed in the KARDEX as “See POST order” • If consultant completes POST, MRP must be notified • Copy is offered to patient/SDM • Dictation/note done following POST completion to describe EoL discussion/decisions in detail
1245 deaths audited for POST completion (Jan-Dec 2010) Next of Kin survey: To examine whether uptake of the protocol is associated with higher family-member satisfaction with end-of-life care (response rate 43%; n=529) Convenience sample of 29 clinician interviews to identify barriers/facilitators for initiative Research Evaluation Study Results
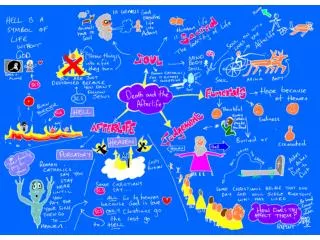
Deaths by month and # with a POST completed 5% 18% 30% 45% 42% 41% 44% 55% 54% 56% 62% 65%
POST Completed by Program 46.1% 34.8% 29.3% 37.2% 59.6% 76.2% 82.4% 59.3%
A death that you could live with… Mary died at age eighty-seven following a brief illness, at home with her family around her. Her relatives loved and cared for her, but she had felt increasingly useless during the last fifteen years of her life. George died at age sixty-nine, working at a job that he enjoyed and from which he refused to retire. He had always wanted to die “in the saddle”, and most people felt this is just what happened. Cal died at age fifty-seven in the hospital after a rather painful illness involving several hospitalizations. He was alerted enough in advance of his death so that he could tie up all the loose ends in his estate and prepare his family for his departure. Edgar died in a nursing home at age seventy-two, six months following the death of his spouse of fifty years. The doctors said he died of a broken heart. Henry was walking out of a downtown bank when he got caught in the crossfire of bullets between police and bank robbers. He was fatally shot, and died immediately on the street at age forty-eight. Betty died at age thirty-seven when the car in which she was riding was struck by a speeding pick-up driven by teenage joy riders. She left a husband of the same age, and two small children. Carrie died at age thirty of an overdose of her antidepressants. She had gone through a series of love affairs, and found that each one left her more depressed than before. Her friends said that what she wanted most out of life was to get married, but she had eventually given up hope, and foresaw only the bleak prospect of life alone. Keith, a single man, died at the age of twenty-three when a kidney which he had received through transplantation failed. He had endured many hospitalizations during his protracted illness but still managed to spread cheer among his family, friends, and the hospital staff who cared for him. (Adapted from R obert E. Neal, The Art of Dying, Harper Collins, 1977 by John O’Connor)
In Conclusion… … helping people plan for the most important trip they’ll ever take