Download
1 / 21
210 likes | 369 Views
The Utility of Evaluating True Vocal Fold Motion Before Thyroid Surgery. Laryngoscope , February 2006 Farrag, Tarik Y. MD; Samlan, Robin A. MS, MBA; Lin, Frank R. MD; Tufano, Ralph P. MD

E N D
The Utility of Evaluating True Vocal Fold Motion Before Thyroid Surgery Laryngoscope , February 2006 Farrag, Tarik Y. MD; Samlan, Robin A. MS, MBA; Lin, Frank R. MD; Tufano, Ralph P. MD From Johns Hopkins University School of Medicine, Department of Otolaryngology–Head & Neck Surgery, Baltimore, MD. R1康焜泰
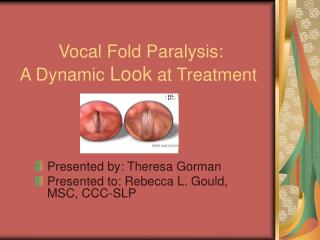
evaluate the utility of screening laryngoscopic examination in evaluating vocal fold (VF) mobility before thyroid surgery.
INTRODUCTION • Thyroid pathologic conditions 11% of the general population. • surgical trauma during thyroid operations recurrent laryngeal nerve (RLN) dysfunction vocal fold (VF) motion impairment
some researchers : up to 50% of patients with unilateral RLN paralysis may be asymptomatic • Rueger RG. Benign disease of the thyroid gland and vocal cord paralysis. Laryngoscope 1974;84:897–907.
use of routine VF examination before thyroid surgery ? • This study • 1. findings in assessing the benefits of VF examination as a routine procedure before thyroid surgery • 2. evaluate impact on the extent of thyroid surgery.
METHODS • retrospective study • 340 patients : thyroid surgery and have had VF examination preoperatively • from January 1998 to June 2005 • 114 males : 226 females. • Age :18 to 87 years • 32.5% (n = 111) indirect mirror laryngoscopy • 67.5% (n = 229) fiberoptic examination or videostroboscopy
Two main categories (based on VF mobility preoperatively • 1) with normal VF mobility • 2) with VF motion impairment
Preoperative diagnosis : • fine needle aspiration • intraoperative condition of RLN • history of previous thyroid surgery • Reports of final postoperative histopathologic examination
RESULTS • Category I (normal vocal fold mobility on preoperative examination; 93.5%, n = 318) • 90% asymptomatic (n = 285) • 10% symptomatic (n = 33) • Fiberoptic or videostroboscopy :214 patients (67%) • indirect mirror laryngoscopy :104 patients (33%)
Category II (vocal fold motion impairment on preoperative examination; 6.5%, n = 22) • seven patients (32%) :asymptomatic without any voice problems (95% confidence interval, 14–55%)
Voice Symptoms as a Screening Test for Vocal Fold Mobility Impairment • Sensitivity was 0.68 (68%)proportion of preoperative thyroid patients with VF motion impairment who were correctly identified as “positive/vocal fold motion impairment” using voice symptoms. • Specificity was 0.9 (90%); this is the proportion of preoperative thyroid patients with normal VF mobility who were correctly identified as “negative/no motion impairment” using voice symptoms
Voice Symptoms as a Screening Test for Vocal Fold Mobility Impairment • Positive predictive value (PPV) was 0.31 (31%); this is the proportion of preoperative thyroid patients with positive voice symptoms who actually had VF motion impairment. • Negative predictive value (NPV) was 0.98 (98%); this is the proportion of preoperative thyroid patients with no voice symptoms who did not have VF motion impairment.
In category II, • 59% (n = 13) malignancy on histopathologic examination • 62% (n = 8) of these malignant cases demonstrated papillary thyroid carcinoma (PTC)
7 patients :asymptomatic +VF motion impairment 5 benign disease on their histopathology reports. • 15 patients: symptomatic + VF motion impairment 11 patients had malignant disease
presence of VF motion impairment plus positive symptoms is strongly suggestive, but not conclusive, of malignancy (P = .07)
differs significantly from the hypothesis that VF motion impairment will only be seen ipsilateral to the thyroid lesion
DISCUSSION • recommend vocal fold examination as a routine preoperative investigation for all patients undergoing thyroid surgery. • 1. high incidence of asymptomatic VF motion impairment (32%) • 2. some patients (10%) with normal VF mobility had positive voice symptoms.
1.asymptomatic + preoperative VF motion impairment majority : slowly progressive benign 2. some cases VF motion impairment contralateral to the side of the thyroid lesion possibility that RLN paralysis independent of the existing thyroid pathology Further diagnostic studies would be needed to explain this possibility
Documenting asymptomatic VF motion impairment preoperatively may provide the surgeon medicolegal protection • Proper preoperative counseling is important, and with preoperative VF evaluation • easier to clearly inform patients about their disease process • explain the risks of thyroid surgery to the RLNs and the resultant functional impairment that comes with injury
CONCLUSION • status of VF mobility is essential information that should be known to both the patient and surgeon before thyroid surgery.