Download
1 / 41
430 likes | 902 Views
Molecular Biologic Markers of Thyroid Cytology. Chan Kwon Jung, MD, PhD Department of Pathology THE CATHOLIC UNIVERSITY OF KOREA Seoul St. Mary’s Hospital. October 22, 2012. Thyroid FNA results. Indeterminate 15-30%. The Bethesda System for Reporting Thyroid Cytopathology.

E N D
Molecular Biologic Markers of Thyroid Cytology Chan Kwon Jung, MD, PhD Department of Pathology THE CATHOLIC UNIVERSITY OF KOREA Seoul St. Mary’s Hospital October 22, 2012
Thyroid FNA results Indeterminate 15-30%
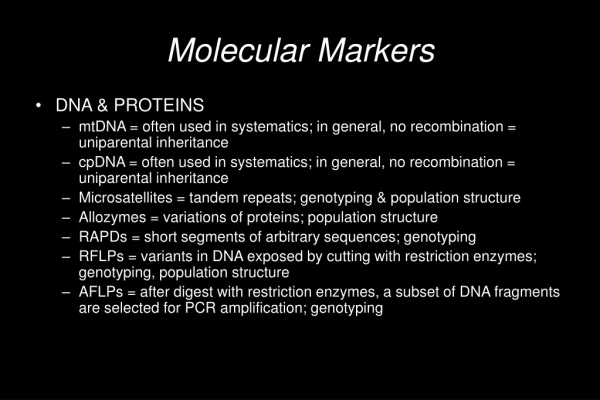
Use of molecular biomarkers • Improve the accuracy of fine-needle aspiration cytology • Provide prognostic information
Genetic alterations in thyroid cancer Activating and inactivating somatic mutations, Alteration in gene expression patterns, MicroRNAdysregulation Aberrant gene methylation
Papillary Carcinoma Papillary Carcinoma TP53 β-catenin PI3KCA PTEN BRAF RAS RET/PTC Follicular cell TP53 β-catenin PI3KCA PTEN TP53 AC PDC RAS TP53 β-catenin PI3KCA PTEN PAX8-PPARγ Follicular adenoma TSHR Gsα Follicular adenoma Follicular Carcinoma Follicular Carcinoma
BRAF mutations BRAF is a serine-threoninekinase. BRAF can be activated by point mutations, small in-frame deletions or insertions, or by chromosomal rearrangement
BRAF Val600Glu (V600E) • 98–99% of all BRAF mutations • papillary carcinoma • poorly differentiated carcinoma • anaplastic carcinoma GTG>GAG c.1799
Prevalence of BRAF mutations in different histologic variants of PTC Xing M. EndocrRelat Cancer 2005;12:245-62
Review of all thyroid FNA studies using the BRAF mutation prior to 2009 * Hyperplasia = atypical nodular hyperplasia Mehta V et al. Head Neck 2012 Sep 13. Epub
Review of all thyroid FNA studies using the BRAF mutation prior to 2009 • 15% to 39% of BRAF-positive FNA samples fell into the nondiagnostic or “indeterminate” categories • Several patients with preoperative benign FNA results were found to be positive for BRAF mutation, and then confirmed as PTC after surgical removal of the thyroid gland • The routine use of BRAF testing would further decrease this false-negative rate. Mehta V et al. Head Neck 2012 Sep 13. Epub
Forward Reverse
BRAF mutation test for diagnosis of malignancy in thyroid FNA *Five false positive cases: 1 FA and 4 NH. Kim SW et al. J Clin Endocrinol Metab 2010;95:3693–3700 Nam SY et al. Thyroid 2010;20:273-279 Yeo MK et al. Clinical Endocrinology 2011; 75, 555–560
False positive • 50 DPO-PCR false positive cases: • false positive rate 1.4%; specificity 98.6% • 3 MEMO-sequencing false positive cases: • false positive rate 0.08%; specificity 99.9% Lee ST et al. J ClinEndocrinolMetab. 2012 ;97:2299-2306
False positive • Ultra-sensitive molecular assays with analytical sensitivity <1% should not be used. • Detection of very low-level mutations can be due to the error introduced during PCR, genetic heterogeneity, and presence of mutation in a very small proportion of cells.
RET/PTC rearrangement 10-20% of papillary thyroid carcinomas RET/PTC1 and RET/PTC3 Various prevalence and specificity: Differences in specific age groups and in individuals exposed to ionizing radiation. Heterogeneous distribution within the tumor Various sensitivities of the detection methods used.
Review of all thyroid FNA studies using the RET/PTC mutation • All RET/PTC positive FNA samples were histologically proven PTCs • No false-positive results • Highly specific biomarker for the diagnosis of PTC
RAS mutations Activating point mutation in codons 12, 13, and 61 of the NRAS, HRAS, and KRAS genes
RAS mutations Follicular thyroid neoplasms, both benign and malignant • 40-50% of conventional type follicular carcinoma • 10-15% of oncocytic type follicular carcinoma • 10-20% of papillary carcinoma almost exclusively the follicular variant • 30% of conventional type follicular adenoma • <10% of oncocytic type follicular adenoma Detection of RAS mutation indicates the presence of a tumor
PAX8/PPARγ rearrangement 30-40% of conventional follicular carcinomas <5% of oncocytic carcinomas 2-13% of follicular adenomas: may be preinvasive (in situ) follicular carcinoma, or tumors where invasion was overlooked or not sampled during examination 1-5% of follicular variant of papillary carcinomas
Molecular testing of FNA samples • Which patients should be tested? • Which biomarkers should be tested? • What is the cost of testing? • How should testing be performed?
Single marker test vsMultimarker panels Korea Western PTC Prevalence 95% 80-90% BRAF (+) rate >80% of PTC 30-50% of PTC
Korean StudiesBRAF mutation test for diagnosis of malignancy in thyroid FNA Sensitivity Accuracy Kim SW et al. J Clin Endocrinol Metab 2010;95:3693–3700 Nam SY et al. Thyroid 2010;20:273-279 Yeo MK et al. Clinical Endocrinology 2011; 75, 555–560
A study with a panel of mutation analyses First two passes Cytologic evaluation Indeterminate: AUS/FLUS FN/SFN SMC 3~4 FNA passes Residual material Molecular analysis: BRAF, HRAS, NRAS, KRAS, RET/PTC1, RET/PTC3, PAX8/PPARγ 400 μL nucleic acid preservative solution Isolation of total nucleic acids Nikiforov YE, et al. J Clin Endocrinol Metab 2011;96: 3390–7
Proposed clinical algorithm for management of patients with cytologically indeterminate thyroid FNA AUS/FLUS (n=212) Cancer risk based on cytology only 14% Thyroid mutation panel (BRAF, RAS, RET/PTC, PAX8/PPARγ) Sensitivity 63% Specificity 99% PPV 88% NPV 94% Accuracy 94% Positive Negative Cancer risk 88% 5.9% Clinical management Total thyroidectomy Lobectomy vs. observation Nikiforov YE, et al. J ClinEndocrinolMetab 2011, 96: 3390-7
Proposed clinical algorithm for management of patients with cytologically indeterminate thyroid FNA FN/SFN (n=214) Cancer risk based on cytology only 27% Thyroid mutation panel (BRAF, RAS, RET/PTC, PAX8/PPARγ) Sensitivity 57% Specificity 97% PPV 87% NPV 86% Accuracy 86% Positive Negative Cancer risk 87% 14% Clinical management Total thyroidectomy Lobectomy Nikiforov YE, et al. J ClinEndocrinolMetab 2011, 96: 3390-7
Proposed clinical algorithm for management of patients with cytologically indeterminate thyroid FNA SMC (n=52) Cancer risk based on cytology only 54% Thyroid mutation panel (BRAF, RAS, RET/PTC, PAX8/PPARγ) Sensitivity 68% Specificity 96% PPV 95% NPV 72% Accuracy 81% Positive Negative Cancer risk 95% 28% Clinical management Total thyroidectomy Lobectomy Nikiforov YE, et al. J ClinEndocrinolMetab 2011, 96: 3390-7
Application of tumor specific mRNA/miRNA expression patterns in FNAC diagnosis
mRNA expression • Microarray studies revealed very distinct changes in the expression of certain genes • No single marker • The aim of current approaches is to identify the minimal number of discriminating genes • Afirma Gene Expression Classifier (Veracyte, South San Francisco, CA) evaluates mRNA expression levels for 142 genes.
Gene Expression Classifier A prospective, multicenter validation study involving 49 clinical centers in the USA: 4,812 FNAs from 3789 patients with thyroid nodules ≥1 cm in diameter over a 19-month period • A gene-expression classifier was used to • test 265 indeterminate nodules • Sensitivity 92% • Specificity 52% • Negative predictive values AUS 95% Follicular neoplasm 94% Suspicious 85% N Engl J Med 2012;367:705-15
Gene Expression Classifier Patients with an indeterminate cytology, but benign gene expression classifier test results have a very low risk of cancer. The test requires two additional needle insertions during FNA biopsy and it is costly.
How much does the molecular test cost? In the USA • Molecular panel testing (BRAF, RET/PTC, and RAS): $650 • Afirma Gene Expression Classifier: $4,200 • Thyroid surgery: $10,00 to $15,000
MicroRNA • small RNA sequences (19–25 nucleotides) that function to regulate the expression of genes • regulate around 30% of the human genome • development, apoptosis, cell proliferation, immune response, and hematopoiesis • tumor suppressor genes and oncogenes
miRs aberrantly expressed in human thyroid carcinomas of follicular cell origin Endocrine-Related Cancer (2010) 17 F91–F104
Summary Benign - Somatic mutation + BRAF or RET/PTC: PTC PAX8/PPARγ: FTC RAS: FTC, FA, fvPTC
Summary Benign gene expression Suspicious