Download
1 / 90
900 likes | 909 Views
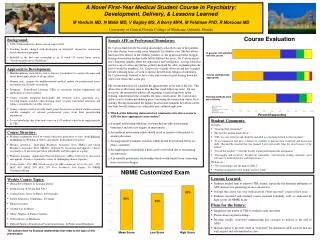
Clinical Utility of Inflammatory Markers and Advanced Lipoprotein Testing: Advice from an Expert Panel of Lipid Specialists. *National Lipid Association Consensus Panel on Biomarker Testing August Orlando, Florida. The Markers. Chairpersons. Authors/Panelists. Presenters.

E N D
Clinical Utility of Inflammatory Markers and Advanced Lipoprotein Testing: Advice from an Expert Panel of Lipid Specialists *National Lipid Association Consensus Panel on Biomarker Testing August Orlando, Florida
Summary Recommendations Abbreviations: Apo = apolipoprotein, CHD = coronary heart disease, hs-CRP = high-sensitivity C-reactive protein, HDL = high-density lipoprotein, LpPLA2 = lipoprotein-associated phospholipase A2, LDL = low-density lipoprotein, LDL-P = LDL particle number, Lp(a) = lipoprotein (a)
Atherogenic Apo B–Containing Lipoproteins VLDL 0.95 VLDL VLDL Remnants VLDL 1.006 IDL Chylomicron Remnants Density, g/mL 1.02 Increasing Density LDL 1.06 1.10 Lp(a) 1.20 15 20 40 60 80 Diameter, nm Adapted from JP Segrest et al. Adv Protein Chem. 1994;45:303–369.
Apolipoprotein B • Does Apo B predict risk over and above traditional risk factors? • What is the physiological rationale for the link between Apo B and adverse CV outcome? • In which patients would Apo B testing be most valuable? • In following up patients who have been treated, does Apo B help in treatment/management decisions? • What are the main areas of controversy regarding Apo B and its use in clinical practice?
Association Between ApoB and CHD Risk VLDL, IDL, and LDL each contain 1 molecule of ApoB; therefore, § plasma ApoB levels reflect the total number of atherogenic parti cles. 1 Epidemiologic studies have demonstrated that apolipoproteins, § including ApoB, may be as good as or often better than LDL - C, non – HDL - C and cholesterol ratios for estimating CHD risk. 1 While non – HDL - C and ApoB are highly correlated and non – HDL - C § has been suggested as a surrogate for ApoB, these 2 parameters can be discordant. 2,3 Correlation between 2 variables assesses how one variable change s relative to the other. 4 Concordance between variables assesses the range of values see n in one variable at a given level of the other variable. 4 IDL = intermediate - density lipoprotein; VLDL = very low - density lipoprotein; ApoB = apolipoprotein B. 1. Chan DC et al. QJM. 2006;99:277 – 287. 2. NCEP ATP III. Circulation . 2002;106:3143 – 3421. 3. Sniderman AD et al. Am J Cardiol . 2003;91:1173 - 1177. 4. Sniderman AD. JAMA . 2005;294:2843 – 2844. 29
ApoB Has Been a Significant Predictor of CHD: Meta - Analysis Results 1 ApoB: Top Third vs Bottom Third AMORIS Dubbo ARIC Women ’ s Health GRIPS Quebec Caerphilly Physician ’ s Health Nurses Health BUPA AF/TexCAPS NPHS2 MONICA - Augsburg ULSAM Reykjavik Kuopio KIHD Guernsey Glostrup – Overall RR = 1.99 (1.65 2.39) 1 2 4 8 N = 6,320 Relative CHD Risk ApoB = apolipoprotein B. 1. Thompson A et al. J Intern Med. 2006;259:481 – 492. 30
Table 1. Meta-analysis of 13 epidemiology studies: overall vascular relative risk ratios (95% confidence intervals) per standard deviation increase Sniderman AD et al. Circulation: CVQO. 2011 4: 337-345
ADA/ACC 2008 Consensus Statement:Treatment Goals in Patients With Cardiometabolic Risk and Lipoprotein Abnormalities aMajor risk factors beyond dyslipidemia include smoking, hypertension, and family history of premature CHD Brunzell JD, et al. Diabetes Care. 2008;31:811-822.
In which patients would Apo B testing be most valuable? • Low Risk • Intermediate Risk • CHD or CHD Risk Equivalent • Premature Family History – ATP III Definition • Recurrent Events
Summary Recommendations: ApoB Abbreviations: Apo = apolipoprotein, CHD = coronary heart disease, LDL-P = LDL particle number,
SUMMARY RECOMMENDATIONS: Apolipoprotein B Initial Clinical Assessment • Low Risk : Not recommended In patients at low risk, the absence of major risk factors and a normal standard lipid profile make the likelihood of markedly elevated Apo B low. Hence, use of Apo B was not recommended in this category . • Intermediate risk, Premature Family History, Recurrent Events : Reasonable for many patients In patients at intermediate risk, those with premature family history, and those with recurrent events, measurement of Apo B would enable the best possible management of modifiable factors for vascular risk • CHD or CHD risk equivalent: Consider for selected patients. Once a patient with CHD or CHD risk equivalent has achieved his or her LDL-C and/or non-HDL-C goals, obtaining an Apo B measurement might be useful for determining whether further intensification of lipid lowering therapy should be considered, as might be the case for discordant individuals with residual Apo B
In following up patients who have been treated, does Apo B help in treatment/management decisions? • Low Risk • Intermediate Risk • CHD or CHD Risk Equivalent • Premature Family History – ATP III Definition • Recurrent Events
Summary Recommendations: ApoB Abbreviations: Apo = apolipoprotein, CHD = coronary heart disease, LDL-P = LDL particle number,
SUMMARY RECOMMENDATIONS: Apolipoprotein B On-Treatment Management Decisions • Low Risk: Not recommended There is no clear benefit of measuring Apo B in patients at low risk receiving lipid altering therapy, and therefore it is not recommended in this group of patients • Intermediate risk, CHD or CHD risk equivalent, Recurrent events : Reasonable for many patients. In patients at intermediate risk, with CHD or CHD risk equivalent, and in those with recurrent events, measurement of Apo B is reasonable for many patients • Premature Family History: Consider for selected patients In patients with a family history of premature CHD, measurement of Apo B should be considered for selected patients
NHANES III Population Percentile Equivalents: Apo B Goals of 90 and 70 mg/dl
LDL-Particle Concentration (LDL-P) • Cholesterol content of LDL particles varies >2-fold between patients, and changes with lifestyle and drug treatment. The result is frequent discordance between LDL-C and LDL-P. • Strong evidence now exists that CVD risk tracks with LDL-P (not LDL-C) in patients with discordant levels. • Discordance analyses show that LDL-C over- or underestimates LDL-related risk in many patients, leading to suboptimal LDL management.
LDL Particle Concentration (LDL-P) • Does LDL-P predict risk over and above traditional risk factors? • What is the physiological rationale for the link between LDL-P and adverse CV outcome? • In which patients would LDL-P testing be most valuable? • In following up patients who have been treated, does LDL-P help in treatment/management decisions? • What are the main areas of controversy regarding LDL-P and its use in clinical practice?
LDL-P Associations Stronger? CHD Status Atherosclerotic Endpoint Study Women’s Health Study Primary Incident MI, CHD YES Prevention death, CVA - Circulation 2009; 119:931-9 Secondary Non - fatal MI or VA - H IT YES Prevention CHD Death Circulation 2006;113:1556 - 63 Primary MESA YES Carotid IMT Prevention Atherosclerosis 2007;192:211-17. Framingham Heart Study Primary Incident CVD YES Prevention Events J Clin Lipidology 2007;1:583-92. Primary Incident C A D EPIC - Norfolk YES Prevention Events Atherosclerosis 2007;49:547-53. Cardiovascular Health Primary Incident MI or YES Study Prevention Angina 2002; 22:1175 - 1180 ATVB Secondary Angiographic PLAC - I YES Prevention MLD Am J Cardiol 2002;90:89-94. Primary EBCT Coronary Health y Women Study YES Prevention Calcium Score Am J Cardiol 2002;90(suppl):71-77i. Published Studies Comparing LDL-C and LDL-P
Relations of Alternate Measures of Atherogenic Lipoproteins with Future CVD Events Framingham (431 events) Values are from multivariable logistic regression analyses adjusted for age, gender, BP, smoking, and lipid rx. Hazard ratios (HRs) are per 1 SD increment of the lipoprotein variable. Cromwell et al. J Clin Lipidol 2007
Event-Free Survival Years of Follow-up Concordant LDL-C and LDL-P in Framingham ( Cromwell et al. J Clin Lipidol 2007;1:583-92) Low Risk Group Low LDL-C Low LDL-P (n=1,249) High Risk Group High LDL-C High LDL-P (n=1,251)
Event-Free Survival Years of Follow-up Discordant LDL-C and LDL-P in Framingham ( Cromwell et al. J Clin Lipidol 2007;1:583-92) Low Risk Group Low LDL-P High LDL-C (n=284) High Risk Group High LDL-P Low LDL-C (n=282)
LDL-C and LDL-P in MESA Relations with CVD Events in Concordant/Discordant Subgroups From Cox regression analyses adjusted for age, gender, and race. Otvos et al. J Clin Lipidol. 2011 5: 105–113
LDL-P LDL-C LDL Size LDL-P > LDL-C 1372 104 20.3 Concordant LDL-P < LDL-C 1249 117 20.7 LDL-C underestimates LDL-attributable risk 1117 130 21.1 nmol/L mg/dL nm LDL-C overestimates LDL-attributable risk LDL-P and LDL-C Discordance in MESA Relations with Incident CVD Events (n=319) 0.06 Cumulative Incidence 0.04 0.02 0 1 2 3 4 5 Follow-up (years) Otvos et al. J Clin Lipidol. 2011 5: 105–113
In which patients would LDL-P testing be most valuable? • Low Risk • Intermediate Risk • CHD or CHD Risk Equivalent • Premature Family History – ATP III Definition • Recurrent Events
Summary Recommendations: LDL-P Abbreviations: Apo = apolipoprotein, CHD = coronary heart disease, LDL-P = LDL particle number,
SUMMARY RECOMMENDATIONS: LDL Particle Concentration (LDL-P) Initial Clinical Assessment • Low Risk: Not recommended Treatment decisions are unlikely to be altered by use of LDL-P among low risk patients. Hence, use of LDL-P was not recommended for this patient group ( • Intermediate risk, Premature Family History, Recurrent Events : Reasonable for many patients There is a substantial number of patients for whom LDL-C may not accurately reflect CVD risk, and data show that discordantly elevated LDL-P is more strongly associated with incident CVD risk than LDL-C. When LDL-P is discordantly elevated, consideration should be given to initiating LDL lowering therapy. Thus use of LDL-P is felt to be reasonable for many patients at intermediate risk (5-20%), those with a family history of CHD and those with recurrent events, all of whom have the potential for discordantly elevated LDL-P • CHD or CHD risk equivalent: Consider for selected patients Due to high CV risk, patients with known CHD or a CHD risk equivalent are candidates for aggressive lipid altering therapy, and it is unclear if additional LDL-P information would alter initial therapeutic decisions, but measurement might be considered for selected patients .
Summary Recommendations: LDL-P Abbreviations: Apo = apolipoprotein, CHD = coronary heart disease, LDL-P = LDL particle number,
SUMMARY RECOMMENDATIONS: LDL Particle Concentration (LDL-P) On-Treatment Management Decisions • Low Risk: Not recommended Treatment decisions are unlikely to be altered by use of LDL-P among low risk patients. Hence, use of LDL-P is not recommended for this patient group • Intermediate risk, CHD or CHD risk equivalent , and Recurrent Events : Reasonable for many patients. Use of LDL-P measurement would be reasonable for many patients at intermediate risk treated to LDL-C and non-HDL-C goal, among patients with CHD or CHD risk equivalents on lipid-lowering therapy, and in those with recurrent CHD events, to adjudicate the adequacy of LDL lowering therapy. When LDL-P is discordantly elevated, consideration should be given to intensifying LDL lowering therapy. • Family History of premature CHD: Considered for selected patients Increased LDL-P is commonly encountered among patients with a family history of premature CHD. Once on therapy, use of LDL-P should be considered for selected patients treated to LDL-C and non-HDL-C goal to adjudicate the adequacy of LDL lowering therapy
Summary Recommendations: ApoB and LDL-P Abbreviations: Apo = apolipoprotein, CHD = coronary heart disease, LDL-P = LDL particle number,
Apo (a) 4 4 4 4 4 4 4 4 4 4 4 4 4 Lipoprotein (a) Lipoprotein (a) Structure Discovered by Kare Berg: 1963 Kringle 3 4 5 2 5 1 Active site (Protease) Plasminogen Apo-B Size heterogeneity (~250-1000 KDa)
Lipoprotein(a) Lp(a) • Does Lp(a) predict risk over and above traditional risk factors? • What is the physiological rationale for the link between Lp(a) and adverse CV outcome? • In which patients would Lp(a) testing be most valuable, if any? • Should Lp(a) be a target of therapy? • How should an Lp(a) measurement affect treatment decisions? • In following up patients who have been treated, does Lp(a) help in treatment/management decisions? • What are the main areas of controversy regarding Lp(a) and its use in clinical practice? • What are the research questions that still need to be answered regarding Lp(a)?
Why is Lp(a) Atherogenic? • Has many of the same pro-atherogenic properties of LDL in regard to cholesterol delivery. • Has structural homology with plasminogen and inhibits fibrinolysis by competing with plasmin. • Inhibits tissue factor pathway inhibitor (TFPI) activity. • May serve as a sink for oxidized phospholipids. • Small isoforms may be more pro-atherogenic.
Lp(a) and CVD Evidence • Over 15 studies have been published, generally showing independent association with CVD • Meta-analyses • Emerging Risk Factors Collaboration - Lp(a) • Erqou et al- apo(a) isoforms • Genetic association- Mendelian randomization studies • 3 Copenhagen studies • Clarke et al NEJM • Prospective and case control studies • Bruneck, EPIC-Norfolk
In which patients would Lp(a) testing be most valuable? • Low Risk • Intermediate Risk • CHD or CHD Risk Equivalent • Premature Family History – ATP III Definition • Recurrent Events
Summary Recommendations: Lp(a) Abbreviations: CHD = coronary heart disease, Lp(a) = lipoprotein (a)
SUMMARY RECOMMENDATIONS: Lipoprotein (a) (Lp(a)) Initial Clinical Assessment • Low Risk: Not recommended. In patients with low risk (0-1 risk factor or 10 yr risk < 5%) Lp(a) measurement can help to reassign patients to a higher level of risk or can help to confirm low risk status if CRP <1.0 mg/L • Intermediate risk or CHD or a CHD equivalent: Consider for selected patients In patients with intermediate risk (2 or more risk factors or 5-20% 10- yr risk) or CHD or a CHD equivalent, it is recommended that Lp(a) measurement be considered for selected patients • Premature family history, Recurrent events: reasonable for many patients Because elevated Lp(a) is additive to CHD risk, measurement of Lp(a) in patients with a premature family history of CHD or in patients with established CHD with a history of recurrent events despite appropriate therapy is a reasonable option
Summary Recommendations: Lp(a) Abbreviations: CHD = coronary heart disease, Lp(a) = lipoprotein (a)
SUMMARY RECOMMENDATIONS: Lipoprotein (a) Lp(a On-Treatment Management Decisions • Low Risk, Intermediate Risk: Not recommended Among patients with low-risk or intermediate-risk for CHD receiving treatment, there is insufficient evidence to support Lp(a) measurement and it is not recommended • CHD or CHD risk equivalent, premature family history, or Recurrent coronary events: Consider for selected patients. Lp(a) measurement may be considered for assistance with on-treatment management decisions in selected patients with CHD (or a CHD risk equivalent), premature family history, or a history of recurrent coronary events, based on the rationale that aggressive LDL-C reduction is beneficial in those with elevated Lp(a) and LDL-C, and that there is no evidence that reducing Lp(a) is harmful.
EAS screening recommendatons for Lp(a) • Premature CVD • Familial hypercholesterolemia • Family history premature CVD or Lp(a) • Recurrent CVD despite statins • ≥10% 10-year risk of fatal/nonfatal CHD