Download
1 / 39
480 likes | 968 Views
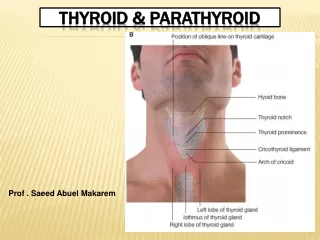
Thyroid and Parathyroid Pharmacology. Thyroid Hormones. Thyroxine (T4, tetraiodothyronine) Liothyronine (T3, triiodothyronine) Iodinated diphenyl ether structure Built and stored on thyroglobulin >99% protein bound in plasma Only free form has physiologic effects

E N D
Thyroid Hormones • Thyroxine (T4, tetraiodothyronine) • Liothyronine (T3, triiodothyronine) • Iodinated diphenyl ether structure • Built and stored on thyroglobulin • >99% protein bound in plasma • Only free form has physiologic effects • T3 more potent; T4 longer lasting • Peripheral deiodination
Physiological Effects • Increases transcription (nuclear) • Increases mitochondrial metabolism • Net effects are target dependent • Oxygen consumption • Heat production • Metabolism, growth, differentiation • Promotes effects of hormones • Steroids, catecholamines
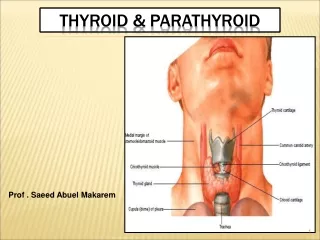
Thyroid Structure Hypothyroid Euthyroid Hyperthyroid
Thyroid Biosynthesis • Iodide Trapping • Thyroglobulin Synthesis • Iodination • Coupling • Proteolysis to release T3/T4 • Deiodination and recycling
Thyroid Gland Regulation + + Hypothalamus Anterior Pituitary Thyroid Gland TRH TSH Adenylyl Cyclase cAMP TSH Receptor - - T3/T4
Hyperthyroidism • Causes • Grave’s disease (TSHR autoantibodies) • 0.1% to 1% prevalence, higher in women • Thyroiditis • Toxic adenoma • Non-pharmacologic treatments • Subtotal thyroidectomy • Radioiodine • Arterial embolization (2005)
Case Report • 47 yo woman reports palpitations, tremulousness, weight loss, heat intolerance of 6 weeks duration • PE reveals HR = 110 bpm, BP = 150/70 a diffusely enlarged thyroid gland, fine tremor of outstretched hands and a wide-eyed stare • Lab reports free T4 = 40 pmol/L, free T3 = 10.6 pmol/L with undetectable TSH and elevated thyroid-stimulating globulins confirming a Dx of Grave’s disease
Hyperthyroidism • Pharmacologic Treatments • Thionamides (thiourelynes)
Hyperthyroidism • Methimazole (Tapazole) • Typical dose 15 – 30 mg QD • Rapidly absorbed (Cmax < 2 hours) • Half-life 13 – 18 hours • Propylthiouracil (PTU) • Typical dose 50– 600 mg BID • Good bioavailability • Half-life 2 – 4 hours • Blocks peripheral T4 -> T3 conversion
Thionamide MOA Coupling is also highly sensitive to drug
Thionamide Side Effects • Rash/itch • Fever • Rarely: • Liver dysfunction • Leucocytopenia
Other Antithyroid Options • Iodide loading • High doses can inhibit iodide formation • Effect transient • May be useful prior to RAI or surgery • Debulk and devascularize gland • Side effects • Rash, hypersalivation, oral ulcers • CI in pregnancy (may cause fetal goiter)
Other Antithyroid Options • Beta Blockers • Adjunctive treatment • May reduce T4 -> T3 conversion • Control HR and palpitations, sweats • Rapid action • Corticosteriods • Reduce T4 -> T3 conversion • May reduce TSHR antibody effect in Grave’s
Case Report • Patient started on PTU 200 mg BIDand propranolol 40 mg TID, becoming euthyroid in 6 weeks whereupon the propranolol was tapered and D/C’d • Remained on maintenance PTU for one year (50 mg bid) then discontinued and remained well for 3 yrs • Symptoms recurred and PTU + propranolol was re-instituted for symptomatic relief. After 7 weeks, she developed a whole body red itchy rash • She received Na131I in a dose of 10 mCi by mouth for definitive control of her hyperthyroidism
Thyroid Storm • Potentially life threatening • Combined treatment strategy • High dose PTU • Give 1st; iodide will reduce drug uptake in gland • Iodide loading (IV Lugol’s solution) • Beta blockers • Corticosteriods
Grave’s Disease Compound “1” TSHRab X + + Hypothalamus Anterior Pituitary Thyroid Gland TRH TSH X Adenylyl Cyclase cAMP TSH Receptor - - T3/T4
Hypothyroidism • Causes • Primary • Idiopathic • Autoimmune • Traumatic • Iatrogenic • Secondary • Pituitary dysfunction • Increased protein binding • estrogen; HIV; liver dysfunction; heroin
Hypothyroidism • Treatment = Hormone Replacement • Synthetic T4 (synthroid) • Absorption fair (65%) • Half-life 5 – 7 days • Synthetic T3 (liothyronine) • Absorption good (>90%) • Half-life 1 – 2 days • Synthetic T4:T3 (Liotrix 4:1 ratio)
Case Report • 3 months later, she returned with lethargy, fatigue, coldness at room temperature, puffiness around the eyes and constipation • Labs showed free T4 = 8 pmol/L, free T3 = 2 pmol/L and TSH = 8 mU/mL confirming hypothyroidism • Levothyroxine 0.1mg daily was instituted and after 6 weeks, blood tests showed a TSH level of 3.2 mU/mL and all symptoms had resolved • She has remained well on this regimen for 2 years
Parathyroid Basics • Parathyroid Hormone • Small molecule (34 amino acids) • Activity based on amino terminal • No disulfide linkages • Encoded on chromosome 11 • Half-life only 2 – 4 minutes • Secreted by chief cells
Calcium Homeostasis • 3 Tissues • Bone • Kidney • Intestine • 3 Hormones • PTH • Calcitonin • Activated Vitamin D3 (1,25[OH]2-D3) • 3 Cells • Osteoblasts • Osteocytes • Osteoclasts
Hypoparathyroidism • Decreased bone resorption & osteocytic activity • Hypocalcemia • Increased neuromuscular excitability • Tetanic muscle contractions/spasms • Seizure • Prolonged QT interval • Cataract • Trousseau Sign • Chvostek Sign • Low or absent iPTH
Hypoparathyroidism • Causes • Surgical (most common) • Idiopathic • Genetic familial forms • Circulating receptor antibodies • Functional • Due to hypomagnesemia • Mg2+ necessary for PTH release
Psuedohypoparathyroidism • Target organs resistant to PTH • Congential defect of PTHR1 • Plasma Ca2+ low • Plasma phosphate high • Renal phosphatase activity high
Hypoparathyroidism • Maintenance Treatment • Combined oral calcium + Vitamin D • Phosphate restriction may be used • Acute Treatment • Tetany or Hungry Bone Syndrome • Parenteral calcium followed by vitamin D supp + oral calcium
Hyperparathyroidism • Primary • Excess PTH high calcium, low phosphate • Tumor, adenoma, hyperplasia • More common in women • Marrow fibrosis • Osteitis fibrosa cystica • Metabolic acidosis • Increased Alk Phos (bone) • Kidney stones
Hyperparathyroidism • Primary – Diagnosis • Multiple elevated Ca2+ serum tests • Elevated iPTH • Alk Phos typically low • Corticosteroid suppression test • Prednisolone reduces serum Ca2+ • Indicates non-parathyroid origin • Sarcoid, vitamin D intoxication, etc.
Hyperparathyroidism • Treatment • Acute Severe forms • Adequate hydration, forced diuresis • Other Agents • Corticosteroids – Blood malignancies • Mythramycin • Toxic antibiotic used to inhibit bone resorption – hematologic and solid neoplasms
Hyperparathyroidism • Treatment • Other Agents • Calcitonin • Inhibits osteoclast activity and bone resorption • Biphosphonates • Given IV or orally to reduce bone resorption • Estrogen • Can be given to postmenopausal women with 1° hyperparathyroidism as medical therapy
Hyperparathyroidism • Treatment • Surgery • Definitive treatment
2° Hyperparathyroidism • Adaptive & unrelated to intrinsic disease of glands • Due to chronic stimulation of glands by low serum Ca2+ levels
2° Hyperparathyroidism • Causes • Dietary deficiency of vitamin D or Ca2+ • Decreased intestinal absorption of vitamin D or Ca2+ • Drugs such as phenytoin, phenobarbital • Renal Failure • Decreased activation of vitamin D3 • Hypomagnesemia