Download
1 / 19
190 likes | 330 Views
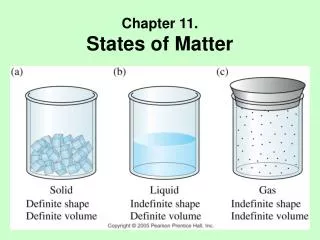
Edematous states & Diuretics. 2 basic steps in edema formation Alteration in capillary haemodynamics that favors the movement of fluid from the vascular space to the interstitium Dietary Na & water are retained by the kidney Major causes of edematous states

E N D
2 basic steps in edema formation • Alteration in capillary haemodynamics that favors the movement of fluid from the vascular space to the interstitium • Dietary Na & water are retained by the kidney • Major causes of edematous states • Increased capillary hydrolic pressure • Increased plasma volume due to renal Na retention: • heart failure • Primary Na retention • Renal ds incl. NS • Drugs: minoxidil, CCB, diazoxide, NSAIDS, fludrocortisone, estrogen • Refeeeding edema • Early hepatic cirrhosis • Pregnancy • Idiopathic edema, when diuretic induced • Venous obstruction • Hepatic venous obstruction, hepatic cirrhosis, • Acute pulmonary edema, Local venous obstruction • Decreased arteriolar resistance • CCB, idiopathic edema • Decreased oncotic pressure (alb<1.5-2mg/dl) • Protein loss: nephrotic syndrome, protein losing enteropathyu • Reduced albumin synthesis: liver disease, malnutrition • Increased capillary permeability • Idiopathic edema, burns, trauma, inflammation / sepsis, allergic reactions, ARDS, DM, IL2-therapy, malignant ascites • Lymphatic obstruction / increased interstitial oncotic pressure • Nodal enlargement due to malignancy • Hypothyroidism, malignant ascites
Renal sodium retention • Inability to excrete the Na & water that has been ingested – patients with renal disease. • Appropriate compensatory response to effective circulating volume depletion, with urine [Na]<25 meq/L • The compensated state • Initial fluid retention has increased venous return to the heart, allowing systemic hemodynamics to be stabilized, and removing the stimulus for continued renin release – noremalization of BP, renin, aldosterone, urine [Na] secretion
Intrarenal factors • Reflex activation of the sympathetic nervous system • Activation of RAAS and ADH • Resistance to the action of natriuretic peptides • Altered glomerular haemodynamics • Peritubular forces in PT
General principles of treatment • When must edema be treated? • Pulmonary edema is life threatening and demands immediate treatment • Other edematous states, removal of fluid can proceed more slowly • What are the consequencesof the removal of edema fluid? • Is the retention of Na & water a compensatory response or inappropriate primary Na retention? • If retention of edema fluid is compensatory then removal of this fluid with diuretics should diminish the effective circulating volume.- decrease in venous return to the heart, and cardiac filling pressures – fall in cardiac output • Leads to increased secretion of the hypovolemic hormones: renin, norepinephrine, ADH. • Most patients will benefit from the appropriate use of diuretics • Adequacy of tissue perfusion can be estimated by monitoring BUN & plasma [Cr] – as long as these parameters remain constant, it can be assumed that diuretic therapy has not led to a significant impairment in perfusion to the kidney or, therefore, to other organs. • How rapidly should edema fluid be removed? • Fluid that is lost initially comes from the plasma; restoration of plasma volume is by mobilization of edema luid into the vascular space • In patients with generalized edema due t heart failure, nephrotic syndrome, or primary Na retention, the edema fluid can be mobilized rapidly, since most capillary beds are involved • Important exception is hepatic cirrhosis with ascites but no peripheral edema – only 500-750 ml/d can only be removed safely.
Cardiac dysfunction Cardiac output Renal Na & water Retention Blood volume venous pressure EDEMA • Congestive heart failure
HEPATIC CIRRHOSIS & ASCITES HEPATIC DISEASE UNDERFILLING OVERFLOW Hypo- Peripheral sinusoidal albuminemia vasodilatation pressure Renal Na & Water retention Plasma volume ASCITES Splanchnic pooling Effective Circ Volume ASCITES Renal Na & Water retention FURTHER ASCITES
Primary renal Na retention RENAL Na RETENTION Plasma volume Capillary hydraulic pressure EDEMA Pathogenesis of edema in primary renal Na retention, which is most often due to glomerular disease, advanced renal failure, Or the use of potent vasodilators in the treatment of hypertension.
Drugs; • direct vasodilators, minoxidil, diazoxide • CCB, dehydropyridines • Pregnancy; • normal pregnancy is associated with retention of 1000meq Na and 6-8L water • Refeeding edema • Insulin directly stimulates Na reabsorption in PT & perhaps in the loop of Henle & DT • Nephrotic syndrome • Idiopathic edema; • in young menstruating women • May represent a capillary leak syndrome • Dopamine deficiency & impaired hypothalamic function • Diuretic induced edema • Chronic use of diuretics activates Na retaining mechanisms
DIURETICS Site of action Carrier/channel inhibited % filtered Na mechanism excreted Proximal Tubule inhibits Enz. Carbonic Anhydrase modest Acetazolamide prevent NaHCO3 reabsorption Loop of Henle Na – K - 2Cl carrier up to 25% Furosemide Bumetamide Ethacrinic acid Distal tubule & Na – Cl Carrier up to 3 – 5% Connecting segment Thiazides Chlortalidon Metalazone Cortical collecting tubule Na Channel up to 1 – 2% Spironolactone blocks aldosterone receptor in cytoplasm Amiloride Triamterene
Other effects • Loop diuretics • Ca reabsorption in the loop of henle is primarily passive, driven by gradient created by NaCl transport • Increase Ca excretion • Treatment of hypercalcemia; NaCl solution & loop diuretic • Thiazide type diuretic • DT is major site of active Ca reabsorption, independent of Na transport • Increase reabsorption of Ca, similar response occurs in the cortical collecting tubule with amiloride • Useful in treatment of kidney stones due to hypercalciuria • K-sparing diuretics • Aldosterone sensitive Na – channel • Can lead to hyperkalemia and metabolic acidosis • Trimetoprim at very high doses • Amiloride in the treatment of lithium induced nephrogenic DI • Triamterene is a potential nephotoxin; crystalluria, cast formation, triamterene stones • Acetazolamide • Net diuresis is modest; reclaimed in the more distal segments, diuretic action limited by the metabolic acidosis • Major indication: as a diuretic in edematous patients with metabolic alkalosis • Mannitol • Osmotic diuretic, inhibiting Na & water reabsorption in PT, loop of Henle • Produces a relative water diuresis, water is lost > Na & K • Can cause increase in plasma osmolality;- can lead to water deficit and hypernatremia, hypertonic mannitol may be retained in patients with renal failure
Determinants of diuretic response • Site of action of the diuretic • Presence of counterbalancing antinatriuretic forces, AII, hypotension. • Rate of drug excretion • Most diuretics, particularly the loop diuretics, are highly protein bound • Are poorly filtered, and enter the urine primarily via the organic – anion/cation secretory pump in PT • Their ability to inhibit Na reabsorption is in part dose - dependent • The natriuretic response tends to plateau at higher rates of diuretic secretion
General guidelines • Use the minimum effective dose • Use for as short a period of time as necessary • Monitor regularly for adverse effects • Use only for appropriate conditions