Download

1 / 18
280 likes | 1.12k Views
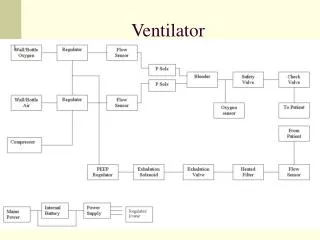
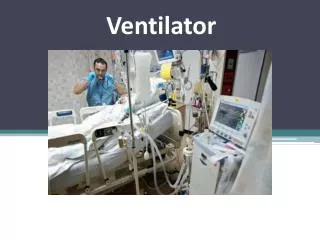
Mechanical Ventilator. Definition. Mechanical ventilation is a method to mechanically assist or replace spontaneous breathing . A ventilator is a device used to provide assisted respiration and positive-pressure breathing.

E N D
Definition • Mechanical ventilation is a method to mechanically assist or replace spontaneous breathing. • A ventilator is a device used to provide assisted respiration and positive-pressure breathing. • Mechanical ventilation is the use of mechanical device (machine) to inflate and deflate the lungs
Indications: • General anesthesia. In anesthetized patients spontaneous respiration may be decreased or absent due to the effect of anesthetics, opioids, or muscle relaxants. • Diagnostic manipulations of the airways such as bronchoscopy. • Comatose or intoxicated patients who are unable to protect their airways. • Endoscopic operative procedures to the airways such as laser therapy or stenting of the bronchi. • Patients who require respiratory support, including cardiopulmonary resuscitation
Impaired in muscles as : • Muscular dystrophy • Damage to the brain respiratory centers • Myasthenia gravis • Myopathies affecting the respiratory muscle • Airway obstruction: • Respiratory failure • Traumatic patient • Acute lung injury (including ARDS, trauma) • Apnea with respiratory arrest, including cases from intoxication • Chronic obstructive pulmonary disease (COPD)
Types of mechanical ventilators include: • Transport ventilators. These ventilators are small, more rugged, and can be powered pneumatically or via AC or DC power sources. • ICU ventilators. Many ICU ventilators also incorporate graphics to provide visual feedback of each breath. • NICU ventilators. Designed with the preterm neonate in mind, these are a specialized to deliver the smaller, more precise volumes and pressures required to ventilate these patients.
procedure and skills of the Mechanically Ventilated Patient Equipment Artificial airway. Mechanical ventilator. Suctioning unit. Preparatory phase Obtain baseline ABG. Chest x-ray Vital signs Give a brief explanation to the patient.
Performance phase Establish the cuffed airway. Prepare the ventilator. -- set up the circuit. -- connect the oxygen and the air. -- turn on the power. -- set the vent. Mode, Parameter. connect vent. To the air way. assess bilateral chest movement. Set the vent., alarm for high, low pressure. Assess ABG. Positioning: -- change from lateral right side to left side every 2 .hrs. -- sit the patient upright to assess lung compliance. -- consider prone positioning to improve oxygenation.
-- Follow sterile suctioning technique every 2 hrs. -- Carry out passive range of motion. -- Assess breath sound every 2 hrs. using stethoscope for the top ad bottom of the lungs. -- check the humidification of the vent. System. -- check theETT cuff pressure. -- observe section condition. -- assess cardiovascular status. -- assess the need for sedation.. -- monitor GIT for blood in stool, haematemsis and abdominal distention. -- provide communication methods as needed. -- provide psychological support. ----- provid documentation sheet for vent. Parameter changes, ABG, Sedation………
Sterile Suctioning • Suctioning consists of inserting a sterile suction catheter into the airway in order to remove secretions. This is an extremely important part of caring for a patient with an artificial airway since the normal reflex of coughing to expectorate secretions is not effective. • Suctioning should be performed only when the patient needs it; however, the need should be assessed at least every two hours. • Sterile technique should be used to decrease the risk of infection. There are now closed suction systems available that are attached to the ventilator tubing on one end and to the artificial airway on the other. The catheter remains protected inside a sterile plastic sleeve and is changed every 24 hours, thus reducing exposure of the trachea to environmental contaminants.
Suctioning causes oxygen deprivation for the time that the suction is applied……. Hypoxemia can be minimized by pr- oxygenating the patient with 100% oxygen prior to suctioning and between each pass of the suction catheter. • The patient’s pulse oximetry should be monitored while suctioning. • The duration of each suction pass should be limited to ten seconds and the number of passes should be limited to three or less if possible. • Studies have shown that using intermittent suction is no more beneficial than continuous suction.
Installation of a small amount of saline prior to suctioning was a common procedure in the past. But.. research has shown this to be a false assumption, that saline installation has been shown to increase infection rates and to cause decreased oxygen levels
Weaning Criteria ---- Obtain ABG. --- Obtain chest x-ray. --- Stable Haemodynamic status. --- The underlying diseases is reversed. --- Ensure adequate neuromuscular control to perform adequate ventilation.
Weaning difficulties factors Acid- base abnormality. Electrolytes abnormality. Fever. Infection. Pain. Sleep deprivation. Unstable haemodynamic status. Alexender, et al,.2007. Nettina, S. 2007.
--- Position the patient well upright as poosible. --- explain the procedure to yht patient. --- ensure no mor esedation is given. --- Et. And Oral suctioning…. And then remove the ETT. --- ensure immediatr oxygen via mask. --- observe vital signs. --- observe o2 sat. Clear the oral secretion. --- ask the patient to coughand regular deep breathing post extubation. --- auscultate the chest. --- apply Pain control. Extubation